



Introduction
Problem Description
Operation Last Resort (OLR) is a performance improvement project that emerged due to not only state regulatory changes, but also the data reflected throughout the facilities around the number of mechanical restraints. OLR is a Belmont Behavioral Health System initiative that highlights the following philosophy with the goal of eliminating mechanical restraints:
Derived from Philosophy of Restrictive Interventions, Belmont Behavioral Hospital (February 2020)
Belmont is committed to promoting a safe environment for both PRS [person’s receiving services] and staff. Therefore, we have made restrictive interventions, such as manual holds; chemical restraints; and in exceedingly rare cases, mechanical restraints, available as a final recourse to maintain the safety of PRS and staff in the treatment milieu. Nevertheless, we recognize that these interventions—especially hands-on interventions and mechanical restraints—are high risk. Their risks and benefits must be weighed carefully with every use.
We believe that:
-
Regular restraint use is not “standard of care” and should be considered a strategy that requires careful consideration and consent, in the same fashion as other medical interventions.
-
Use of a restraint is the last resort and should evidence exhaustion of all other methods of de-escalation on the part of the PRS’ treatment team.
-
For a traumatized population, the risks of a restrictive intervention will most often outweigh the benefits, and may escalate a situation or rupture a relationship with a treating team.
-
Reducing restraint usage is the responsibility of every direct-care or clinical team member and leader.
Utilizing the Six Core Strategies for Reducing Seclusion and Restraint Use, the facility developed a strategic action plan outlining OLR.1
Rationale
Restraint is defined as the use of a physical or mechanical device, material, or equipment that immobilizes or reduces the ability of a patient to move their arms, legs, or body freely. The Joint Commission and Office of Mental Health and Substance Abuse Services mandate that restraints may only be used for the management of violent or self-destructive behavior that jeopardizes the immediately physical safety of the patient, staff, or others. It may only be used after less-restrictive interventions are ineffective or ruled out.2,3
Mechanical restraint includes the restriction or limitation of body movement by use of bed restraints (up to four points) in a bed with appropriate restraint structure. Physical restraint does not use straps or other mechanical structures. It involves a physical “hold” by trained staff who are able to intervene quickly and end the hold immediately when the patient has calmed and is no longer a danger. Physical restraints tend to be in use for a shorter duration than mechanical restraints and although they are used primarily with children, adolescents and adults were also in scope for this intervention.
A review of previous attempts toward restraint reduction at Belmont revealed two primary barriers. The first was the resistance of direct-care staff who were reluctant to part with a tool they believed secures safety. The second was an absence of full training and real-time support to demonstrate for staff that there are alternative tools that not only are less harmful, but also can yield positive clinical outcomes.
The Six Core Strategies are well-known, best-practice approaches to reducing the use of restraints through organizational change, data-informed practices, workforce development, and consideration of consumers’ roles in their own care. They have been used by behavioral healthcare providers to successfully decrease or eliminate restraints and were adopted by Belmont as a guide and philosophy to support this project.1
Lewin’s three-step model of change (unfreezing, changing, and refreezing) supported the process of confronting staff apprehension about letting go of mechanical restraints as a treatment tool and embracing new interventions. These steps were taken to determine what areas in this process required more education/training and whether leadership was holding accountability, and moving forward to ensure the changes are “refreezing” and ultimately improving patient outcomes. Change can be difficult and meet resistance, but providing the organization with projected goals and ongoing review of progress and sustainability is the focus in this performance improvement project.4
The Plan-Do-Study-Act (PDSA) cycle used to measure progress of change is outlined in this paper. The “planning” started with the opportunity for improvement identified within the psychiatric clinical environment in the use of four-point mechanical restraints. During planning the organization developed a plan based on the Six Core Strategies and developed an organizationwide statement that reflects its belief that utilization of mechanical restraints is a failure in clinical practice. To “do” this, the organization utilized evidence-based practice through research and clinical practice guidelines that can improve and support change that will improve clinical care outcomes. Data was identified to show the use of four-point mechanical restraints over time and areas where improvement was needed. When “studying” this project, it is important to identify all aspects of the project during monthly leadership meetings to show that commitment to the project is ongoing and improvement is taking place. Finally, the “act” cycle for this project will show whether “refreezing” is taking place, whether the measurement tools identify progress in the right direction, and what changes if any need to be implemented.
In summary, this quality improvement project identified processes, structures, and patient outcomes related to restraint reduction within the organization. Each opportunity for improvement included a needs assessment for the identified barriers. The action steps necessary to implement change and accomplish the goal of reducing the use of four-point mechanical restraints in hospitalized patients were guided by trauma-informed care and the Six Core Strategies, in turn decreasing physical and psychological injuries and improving patient care.
Integrating Lewin’s change model into the PDSA cycle provided the ability to pivot in response to the needs of the staff and patients as the project moved forward. The combination of following the data and tracking the needs of staff/patients on a daily basis was key in allowing staff to feel supported and encouraged by the success of their efforts. Consistent reinforcement and appreciation by hospital leadership further enhanced the positive movement toward the culture change sought for this project.
Available Knowledge
There is a consensus in the literature that mechanical restraints are harmful to patients who are subjected to them. Individuals may experience retraumatization, fear, powerlessness, and sometimes even physical injury. The literature reflects safety being a key component to why mechanical restraints could be necessary. The weighing of patient trauma and safety (patient safety, staff safety, and environmental safety) is a difficult decision for many, especially in moments of crisis. Many studies do indicate positive results from other forms of noninvasive means to crisis de-escalation but also indicate need for more studies to systemize or methodize these approaches, as they are contextual, ever-changing, and individualized. OLR is aimed to support filling this gap in literature and support the mental health field in providing a trauma-informed approach that does not weigh patient trauma against safety of patients and staff in moments of crisis.5–7
Context
Belmont is currently a 252-bed acute care psychiatric hospital located in Philadelphia. Approximately 80% of patients admitted are insured by Medicaid or Medicaid managed care insurance. Over the time of this project, Belmont transitioned from a 180-bed facility into a brand-new facility with a 252-bed capacity. The census was titrated over a six-month period until March 2022, when an autism specialty unit was introduced and bed capacity was fully implemented. Belmont provides care for individuals with ages ranging from 5 and up but does not have an age limit for adult patients. Approximately 60% of patients were over 18 years of age. The age range is not static, due to seasonal fluctuations, but the percentiles did not vary markedly through the calendar years and building occupation transition.
Specific Aims
How does the use of trauma-informed care techniques help reduce the utilization of restraints compared to use of mechanical restraints, and overall reduce the number of injuries and psychological trauma that may be endured? Utilizing SMART (Specific, Measurable, Achievable, Relevant, and Time-Bound) criteria to show the quality improvement goal will indicate:
Specific: The overall goal is to reduce the use of mechanical four-point restraints, as their use is known to affect patients adversely: physical injuries, psychological trauma, and deaths have been reported. The use of mechanical restraints causes traumatization and retraumatization.
Measurable: Review of the data related to mechanical restraint utilization and clinical evidence supporting reduction and eventual elimination of mechanical four-point restraints.
Achievable: Primary prevention principles based on trauma-informed care and strength-based approaches are key elements of treatment, such as the Six Core Strategies.
Relevant: Review of current utilization of four-point mechanical restraints reflective of patients being served, noncompliance with hospital policy, staff discomfort/concern with minimizing utilization of four-point mechanical restraints, and adapting to trauma-informed care and the Six Core Strategies to reduce these numbers.
Time-Bound: Reduce the rate of four-point restraints in patients by 50% over the next 12 months with an ultimate goal of 100% over the next 24 months.
Methods
Interventions
Interventions were developed using the Six Core Strategies framework:1
1. Leadership Towards Organizational Change
Reduction of mechanical restraint use had been a goal of Belmont leadership. In choosing an overarching strategy that was guided by leadership, the goal was not to remove a tool but to add to the tools available through-trauma informed care and de-escalation strategies.
The project was named “Operation Last Resort” (OLR) to drive the concept that mechanical restraint was not a treatment, but a failure of treatment. The challenge to reducing staff dependence on mechanical restraint was to address the underlying fear that without it patients and staff were placed at risk. The strategy for dissolving that fear was understood to be a process and needed to occur in incremental steps building confidence and skills with every phase.
Belmont leadership made a visible commitment to staff of the importance of this change by making investments in training and education, as well as feet-on-the ground support by members of leadership. Executive and Nursing Leadership Team committed to the same de-escalation and training as direct-care staff. A representative from Leadership responded to every aggression/behavioral code. Following all aggression or behavioral codes, the most senior leader was required to lead all staff participating in the code through a staff debriefing session immediately following the code. To ensure accountability, all episodes of utilization of mechanical restraints require a notification to a member of senior leadership.
2. Using Data to Inform Practices
Both qualitative and quantitative data usage are outlined in the Measures section of this paper.
3. Workplace Development
Belmont’s philosophy of using the least restrictive intervention was formally developed, shared with staff, posted on all units, included in the patient handbook, and emphasized in new employee orientation.
A campaign was developed to draw attention to the changes. This included informational pamphlets, education-oriented staff meetings, and other handouts. A full-day kickoff event that touched all shifts occurred where staff signed a banner pledging to Operation Last Resort, which was hung prominently in the hospital lobby. A bulletin board in the employee hallway was dedicated to restraint reduction and a large countdown sign was installed to mark every restraint-free day. Staff members who demonstrated effective usage of nonrestrictive interventions with strong ability to use trauma-informed care and de-escalation were rewarded as “Restraint Reduction Champions.”
Training
Staff already demonstrating skills in de-escalation and leadership were selected to become Therapeutic Options (TO) trainers.8 Trainers were paired into “training partners” who represented both direct-care staff and clinically trained staff to provide the most appealing education to the various roles represented throughout the hospital.
The leadership model throughout this rollout time was an interdisciplinary approach in which all departments were asked to have active engagement on the floor with staff in real time. This approach went beyond nursing and behavioral technician levels of care, to include members of the Social Services and Clinical Services departments not traditionally included in restraint activity. The value of interdisciplinary cohesion was endorsed, resulting in a stronger buy-in from direct-care staff. Engaging both allied therapies and leadership resulted in perspective change demonstrating that no one was alone in the process. The leaders who supported these changes demonstrated that they were truly engaged in the initiative and motivated to see the process and culture change.
A multilevel approach to training included:
-
Skills clinics held along with TO recertification
-
Skills fairs were held to reinforce training
-
Leadership-focused qualitative data derived for staff interviews/feedback
-
Public recognition of staff who demonstrated investment in the process through the institution of a monthly Restraint Reduction Champion award
Current and new staff received:
-
Eight hours of verbal de-escalation training
-
Eight hours of TO training related to physical restraints
-
Sensory room and sensory-based de-escalation training was provided to all current staff and in new-hire orientation
-
Child and adolescent de-escalation training was provided in new-hire orientation
-
Trauma-informed care training was provided in new-hire orientation
-
Child-adult relationship enhancement training grounded in parent-child interaction therapy was provided in new-hire orientation

4. Use of Restraint Reduction Tools
Therapeutic Options (TO) is a trauma-informed care de-escalation approach that uses “positive behavior supports” to support mindfulness and respect toward individuals experiencing crisis or emotional dysregulation.
“The ultimate purpose of Therapeutic Options training is to build our capacity to be with people in a meaningful way; to be a source of healing, encouragement, and safety to everyone who comes to us for help, no matter how challenging their behavior or complex their support needs.”8
As well as tools to support self-regulation for the patients, Belmont recognized the importance of a physical environment that reflected calm. Occupational therapists created “sensory rooms.” These spaces provide a safe, de-escalation space for patients. Use of the room is encouraged but completely voluntary and not for seclusion. The rooms provide a proactive, crisis prevention tool for staff that can be used to assist patients to manage their symptoms and behaviors. Individualized referrals for verbal, visual, music, and art therapies were made available. Peer specialists, board-certified behavior analysts, and occupational therapists were referred to on a case-by-case basis to support acuity and provide additional support for patients struggling to regulate their emotions. Individualized behavioral plans were created to enhance behavioral management programming across all child and adolescent programs.
5. Consumer Roles in Inpatient Settings
Informal qualitative interviews were completed for both the patient and involved staff after each mechanical restraint episode. As themes emerged from these interviews, they were used to refine skills and develop action plans. Content was integrated into skills clinics that occurred during the second half of TO recertification days. During those times trainers either held small open house sessions with staff off the floor or went from floor to floor or department to department. This time was used to provide education or demonstrate methods to safely address the themes that arose during the qualitative interviews.
As a part of our clinical services department we also have a peer support specialist who is available to provide consultation to staff or peer support from their own perspective.
6. Debriefing
Debriefing following an episode of restraint is required by Belmont policy and expected after every restraint episode. There is a Debriefing Form to guide the process. This expectation was prioritized and leadership was given accountability to ensure that it did occur. Leaders were trained on debriefings, with a focus on identifying positives as well as opportunities for improvement. Patients were also provided the opportunity to debrief with a staff member who was not a participant in the restraint.
Following debriefings, relevant findings and recommendations were added to treatment plans and reviewed with the primary treatment team. For patients with more than one restraint during a week, a more intensive review was completed with relevant staff, including behavioral specialists. Additionally, staff debriefings became a standing agenda at all nursing department meetings.
Study of the Intervention
An intensive examination of intervention effectiveness and outcomes was ongoing across a number of internal meetings, allowing for multiple perspectives and diverse feedback. The Restraint Reduction Committee reviewed data monthly, which included time of day, shifts, and patient specificities. Unit activity during the time of the codes and staffing levels were also considered. From a more qualitative perspective, interventions of individual staff members and review of medication management, near misses, and the successful interventions were open for discussion. Episodes were also reviewed with the full treatment team. Outliers with more than one mechanical restraint were reviewed in the “Acuity Meeting” and with members of leadership.
In preparation for transition to the larger facility, the Restraint Reduction Committee did a safety risk assessment of the new facility based on restraint risk. The building was designed with high reliability as a priority, so the wings of all four patient care floors were designed to be either identical or mirror images of each other. This helped to mitigate risk from the additional challenge for staff not familiar with the layout of the new setting. Concerns about code response times/routes, new restraint beds, safety risks, etc. were evaluated. When concerns arose, the committee worked closely with the hospital Command Center Team to identify solutions that would better support patient safety. At the time of the move, the transition to restraint-free was not fully completed, therefore the new facility had to accommodate mechanical restraint activity. One finding of the committee was that the newly purchased mechanical restraint beds were not trauma-informed and did not fit the current mechanical restraints in use. As a result of their findings, the committee was able to ensure that the beds were retrofitted for trauma-informed care.
Measures
Ethical Considerations
Safety for staff and patients throughout this process was the primary consideration. An increase in injuries was an unacceptable outcome. To mediate this risk, the process was purposely slow and moved incrementally, measuring outcomes daily. Review of data indicates that there was no increase in patient-related injuries between 2021 and 2022.
Results
In 2021, Belmont Hospital made a full commitment to the elimination of mechanical restraints in the acute care inpatient setting. Restraint reduction was a primary quality initiative for multiple years without success. An analysis of previous attempts toward restraint reduction at Belmont revealed two key barriers. The first was the reluctance of direct-care staff to part with a tool believed to provide safety. The second was an absence of trauma-informed alternative tools that were less harmful and could yield positive clinical outcomes.
Adopting the Six Core Strategies for Reducing Seclusion and Restraint Use, the goal of this project was to implement an evidence-based practice that would identify barriers and support staff in the use of techniques that reduced trauma and restraints.
Progress toward zero mechanical restraints was incremental. Both qualitative and quantitative data were used on a daily basis to support staff interventions. Active investment from leadership and allied professions provided support for a culture shift that went from using mechanical restraint almost daily to a culture where mechanical restraint is seen as a failure. This success was sustained through 2022 and is now a standard expectation for care at Belmont.
Discussion
Summary
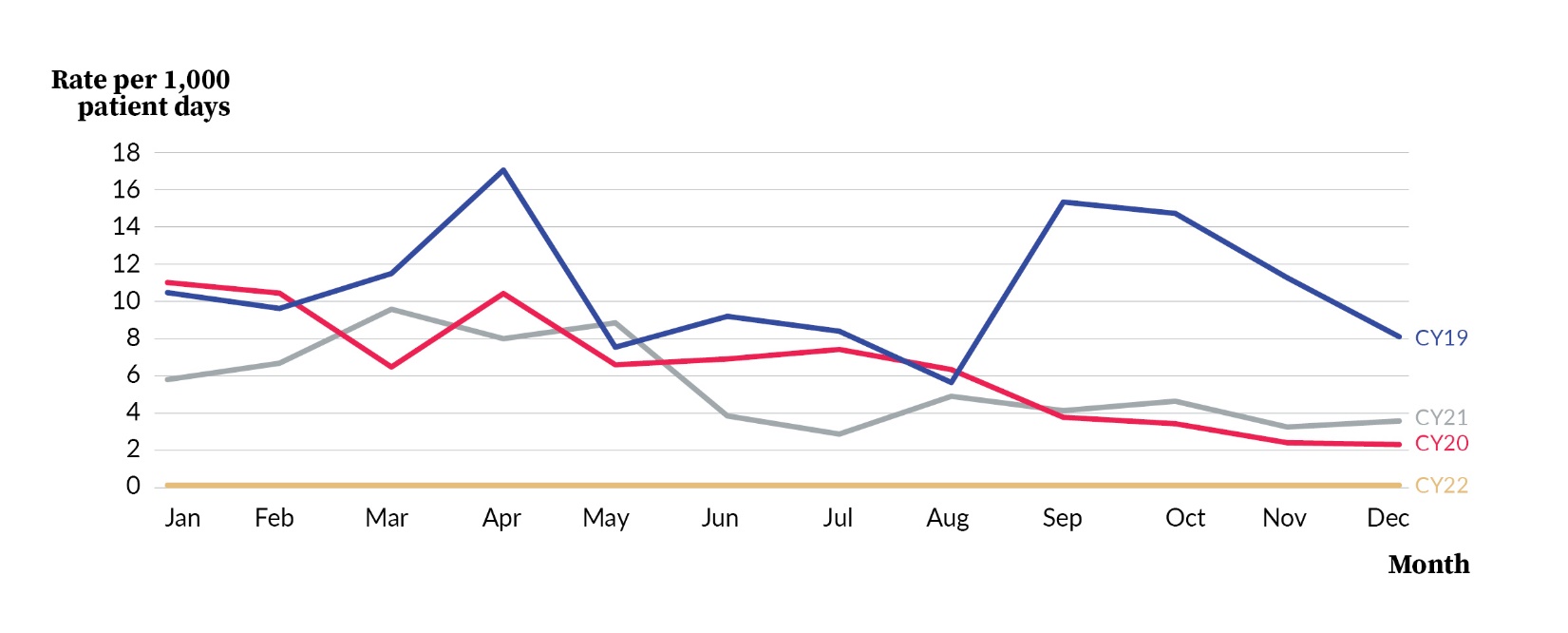
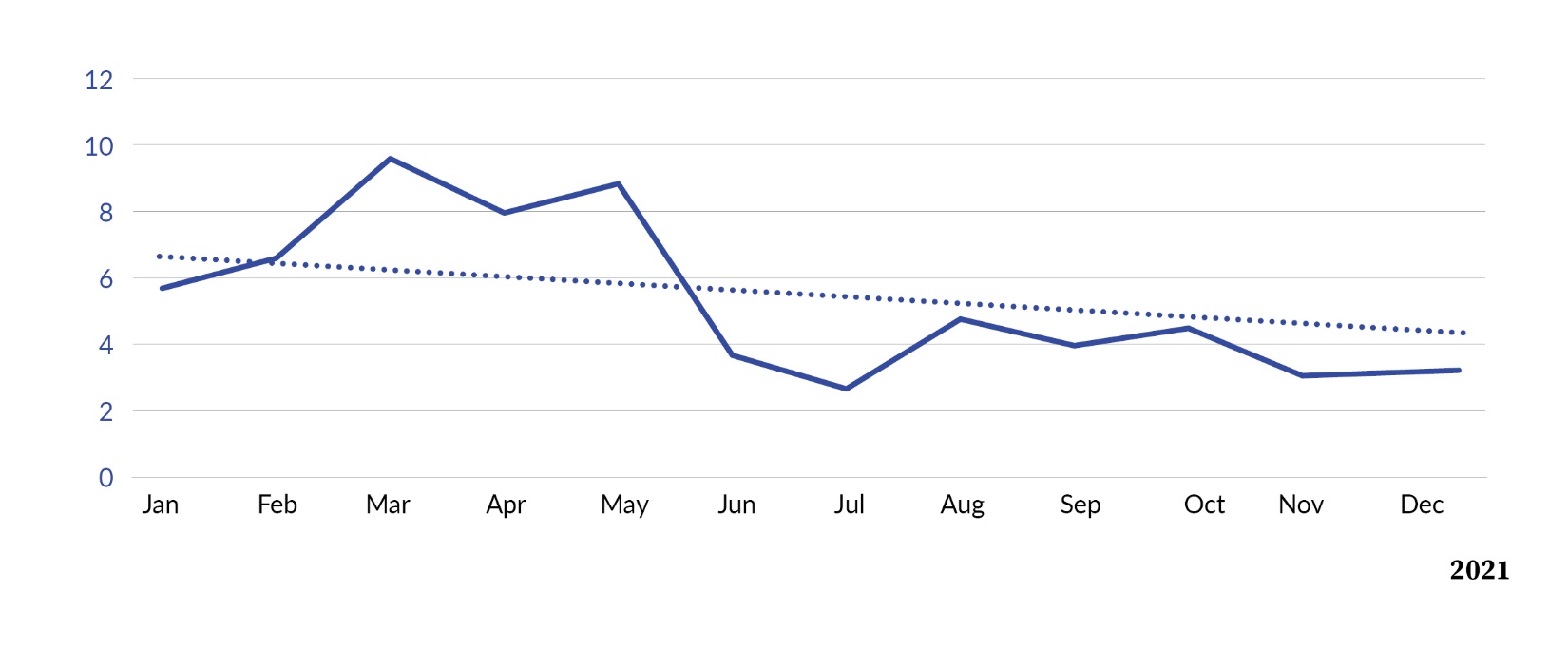
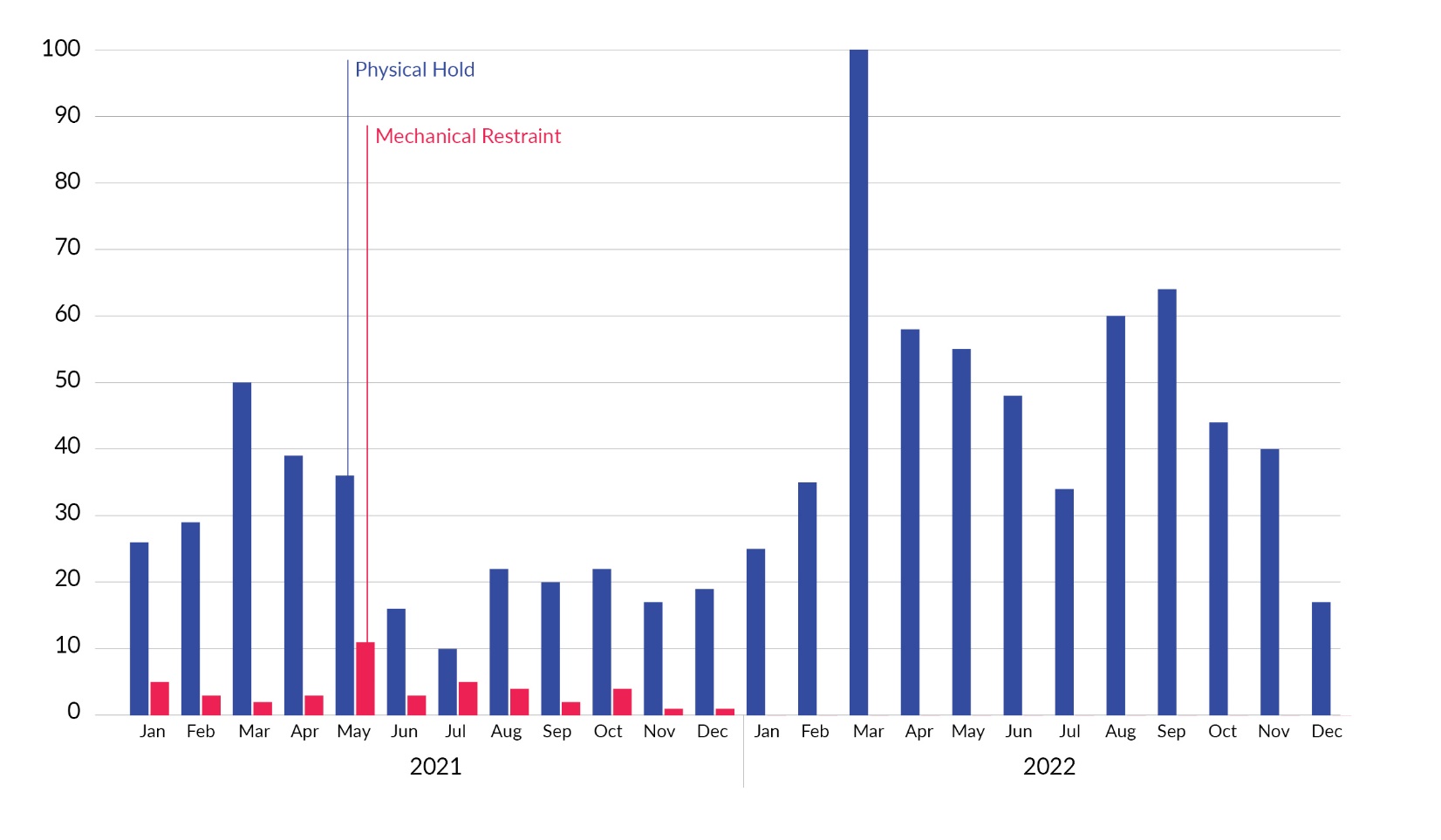
Based on a strategy of slow, incremental steps, Belmont was able to gradually reduce and finally eliminate mechanical restraints in the inpatient setting. The year-over-year progress of restraint reduction efforts was uneven and unsuccessful from 2019 through 2020 (see Figure 1). During 2021, the number of restraints was reduced until the facility reached zero mechanical restraints after December 5, 2021 (see Figure 2). Zero mechanical restraints continued through 2022, signifying sustainability (see Figure 3). As a result, it was possible to completely remove mechanical restraint equipment from the facility. 2022 saw a rise in the rate of physical restraint use to 15.75 in March, but by December the value was 2.62, the lowest point in the entire year (see Figure 4). Also noted, there was no measurable increase in staff injuries during or following the transition.

.jpeg)
.jpeg)

Interpretation
Belmont is not the first inpatient setting to eliminate restraints for its programming. This project provides additional evidence that a restraint-free inpatient setting is possible with sufficient investment in staff and training. Using trauma-free interventions was an additional quality benefit that is believed to have enhanced the advantages of the way this program was designed. The implementation of this model and supporting interventions can provide a roadmap for other programs seeking to enhance the inpatient experience for both staff and patients.
Strengths and Limitations
The biggest strength that was reflected throughout this entire process was the ability for all disciplines and team members to come together and achieve a shared goal. The pandemic caused all of our departments to get specific scrubs per discipline; besides comfort and infection control, this organization of departments allowed the committee to see what disciplines were most present for codes, as well as who needed additional training and support. The biggest impact was the sea of all colors responding as a united team to effectively support and manage our patients during their hardest moments. The visual of this multidisciplinary effort delivered a powerful message and demonstrated to leadership and staff that the culture was shifting from “control of the environment” and “compliance” to “empowerment” and the intent to provide comfort to the vulnerable populations served by Belmont.
A challenging factor to this initiative was the skepticism from frontline staff and some leadership members. To change a deep-rooted, habituated process and promote a culture of providing services in the mental health field, people had to see to believe. This put immense pressure on leaders to lead and show investment throughout all de-escalation episodes.
Conclusions
In summary, this project enabled the removal of mechanical restraints from an acute inpatient behavioral health hospital servicing children, adolescents, and adults. The factors that supported the success of this project were true endorsement from leadership, robust staff training, and continuous feedback and supervision. Through these factors, sustainability over at least one year was achieved.
Funding
There were no external funding sources for this project.
Acknowledgements
The authors would like to sincerely thank Jennifer Polen, LCSW, for being an integral part in launching the OLR initiative and chairing our Restraint Reduction Committee. Special thank you to Christopher Wilson MSN, RN, for strategically outlining the action plan utilizing the Six Core Strategies and co-chairing our Restraint Reduction Committee.
Lastly, acknowledgement to Laura Longstreet, Acadia Healthcare Group chief executive office, Pennsylvania Market, for believing in the vision and supporting OLR every step of the way. Her leadership and belief in all staff at every level of the organization raised the bar of accountability and empowerment, making this possible.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
Dawn Bausman has worked in the mental health field for over 13 years and is currently the chief nursing officer at Belmont Behavioral Health System. Bausman earned her Master of Science in nursing from the University of Alabama with a concentration in administration. She assists in developing programs, processes, and protocols that have supported the changing culture of mental healthcare at Belmont.
Shawna Gigliotti (shawna.gigliotti@belmontbehavioral.com) is the director of Training and Development for Belmont Behavioral Health System. She completed her doctorate in occupational therapy from University of the Sciences in Philadelphia.
Margaret Meshok has a Master of Social Service degree and doctorate in social work from Bryn Mawr Graduate School of Social Work and Social Research. She is currently the director of Quality and Regulatory Affairs for Belmont Behavioral Health System.