








Introduction
Thrombolytics (i.e., fibrinolytics) are a class of medications that dissolve blood clots and maintain vascular patency.1,2 Alteplase and tenecteplase are agents in this class that are currently available for the lifesaving treatment of serious conditions such as acute ischemic stroke (AIS), acute myocardial infarction (AMI), and pulmonary embolism (PE).3,4
Alteplase (Activase) is the first recombinant human tissue plasminogen activator approved by the U.S. Food and Drug Administration (FDA) and has been the drug of choice for intravenous thrombolysis since it appeared on the market in 1996.5,6 It is the only agent within the class that is FDA-approved for AIS, AMI, and PE.3 For the treatment of AIS, alteplase requires a weight-based dosing with a bolus administration followed by an infusion over one hour.3
Tenecteplase (TNKase) is a genetically engineered tissue plasminogen activator that has a faster onset of action, longer half-life, and greater specificity to fibrin than alteplase.5–8 It has the additional advantages of a single bolus administration and a lower cost compared to alteplase.9–11 Although currently FDA-approved to treat AMI only, tenecteplase also has been shown to be safe and effective in its off-label use to treat AIS.12–17 Currently, the guidelines for early management of AIS by the American Heart Association and the American Stroke Association suggest tenecteplase as a reasonable alternative to alteplase, with a Class IIb level of recommendation.18
As a class, thrombolytics are considered high-alert medications, meaning that they could cause serious harm to a patient if used in error.19 Alteplase and tenecteplase have been associated with several types of medication errors due to both medications having multidosing regimens, being commonly referred to by abbreviations, and being dispensed from the same care area to treat similar patient populations.20–29 Between October 2000 and June 2014, the FDA received 21 reports of wrong-drug errors associated with tenecteplase.6,30 In 2015, it issued an FDA Advise-ERR to warn against the confusion between alteplase and tenecteplase,28 including the problems caused by using the abbreviation “TPA,” which stands for “tissue plasminogen activator.”20–24,28,31 Despite the aforementioned risks and concerns, we are unaware of any studies that have explored and compared the full range of medication errors occurring with alteplase and tenecteplase during treatment of AIS. (One prior study explored only dosing errors32 and another study explored only wrong-drug errors.29)
The purpose of this two-part study is to measure the frequency of event reports in which either alteplase or tenecteplase was the medication prescribed, regardless of indication, and to further analyze medication errors that involved the treatment of AIS. Based on findings related to the stages of the medication-use process, associated factors, and event types, we aim to identify similarities and differences in the patient safety risks associated with these medications when used to treat AIS. We anticipate that the findings of this study will help staff across multiple disciplines identify gaps in their safety practices and develop strategies to mitigate risks associated with the use of alteplase and tenecteplase to treat AIS.
Part I
Methods I
This study used the Pennsylvania Patient Safety Reporting System (PA-PSRS)[1], which is one of the largest patient safety databases in the world and contains more than 5 million event reports submitted by healthcare facilities across the state of Pennsylvania.33,34 Each PA-PSRS report includes several structured fields (e.g., event date, patient age, patient gender, care area, facility type) as well as free-text narrative fields that the reporter can use to describe the safety event. Due to the unstructured nature of the free-text narrative fields, the quantity and quality of details may vary from one report to another.
For Methods I, we performed a query of the PA-PSRS database “Medication Error” category for reports submitted between January 1, 2017, and December 31, 2022, that used the keywords “alteplase,” “tenecteplase,” and spelling variations of their generic and brand names in the “Medication Prescribed” field. The objective of Methods I was to explore the extent of reported events involving the two medications, regardless of indication, and guide the design of the inclusion criteria for Methods II of the study.
Results I
Methods I generated a total of 858 reports, of which 92% (791 of 858) involved alteplase and 8% (67 of 858) involved tenecteplase (Figure 1). Tenecteplase-related reports had a frequency near zero from 2017 to 2020 and increased in 2021 and 2022, while the number of alteplase-related reports increased in 2018 and 2019 and decreased each year thereafter. As a result of these changes in frequency of reports, we targeted the 2021–2022 time period for further analysis in Methods II.

Part II
Methods II
Based on the findings from Results I, we chose to narrow the scope of Methods II to further examine the nature of events involving alteplase and tenecteplase in the treatment of AIS. As shown in Figure 2, we started with 301 reports from Methods I submitted to PA-PSRS in 2021–2022 and then applied the following inclusion criteria:
-
The report described a medication error, which we defined as “any preventable behavior or condition directly involving alteplase or tenecteplase that created a potential for harm or caused harm to a patient” (adapted from the National Coordinating Council for Medication Error Reporting and Prevention definition35)[2].
-
Alteplase or tenecteplase was intended for the intravenous treatment of AIS[3].

Variables Coded
Each report that met inclusion criteria was coded with two sets of variables. The first set was coded by the reporter at the time of submission to PA-PSRS and included variables such as the event date, care area[4], facility type, and patient demographic information. The second set of variables consisted of the intended thrombolytic medication, near miss, clinical indication, stage of the medication-use process, associated factor, and event type. Each report was reviewed and manually coded by two researchers, and any discrepancies were discussed with a third researcher until consensus was reached. Our coding taxonomies for stage of the medication-use process, associated factor, and event type were developed using a deductive approach by adapting the PA-PSRS taxonomy and prior literature,27,36,37 combined with an inductive approach to create additional codes where necessary.
Near Miss. The event was considered a near miss if it did not reach the patient (i.e., did not impact or interrupt patient care) due to chance or active intervention.
Clinical Indication. A clinical indication was defined as a medical condition or reason to prescribe the thrombolytic agent. Although all the prescribed thrombolytics included in the study were intended for AIS, we also coded clinical indications for which the medications were incorrectly ordered or dispensed. When not explicitly mentioned in the event details, the clinical indications for which the medication was intended, ordered, and dispensed were identified by examining the dose, consult type, methods used to prepare or administer the medication, and other contextual information provided in the report details.
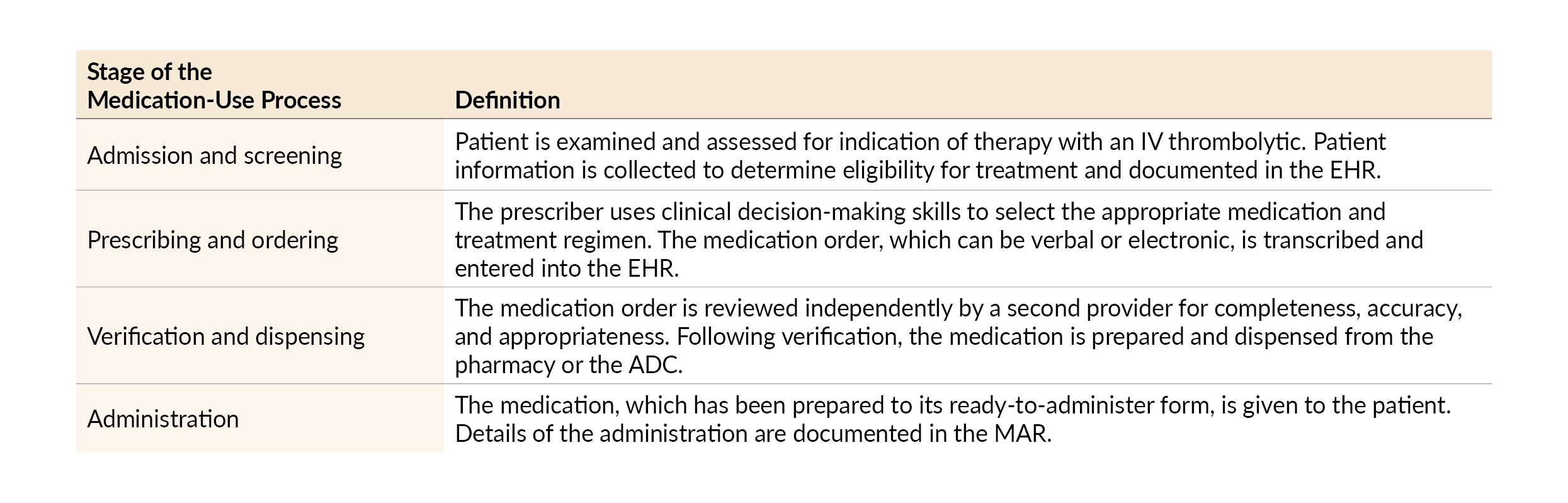
Stage of the Medication-Use Process. See Table 1 for definitions of the four stages of the medication-use process that characterize the chronological order of events and behaviors that typically occur in the acute care setting. We coded event reports according to the following four stages of the medication-use process: Admission and screening, Prescribing and ordering, Verification and dispensing, and Administration. We defined the stage as the point in the medication-use process at which a preventable behavior or condition likely contributed to the safety event (i.e., associated factor; see Table 2).

Associated Factor. An associated factor was defined as the preventable behavior or condition that likely contributed to the safety event. Based on the complexity of the safety event and details provided by the reporter, multiple associated factors may have been coded for a single report. When two or more reports shared the same associated factor, a standalone category of associated factor was formed. We identified 24 associated factors occurring across the four stages of the medication-use process. The associated factor Other contained reports that did not fit into a more specific category of associated factor for that stage. See Table 2 for definitions of the 24 associated factors.

Event Type. An event type was defined as the actual or likely result of the associated factor. One event type was coded for each report. If the report lacked sufficient details or the event was a near miss and had the potential for multiple event types, the event was categorized as Unable to determine. See Table 3 for definitions of the nine event types.

Data Analysis
We performed a descriptive analysis to explore the data and identify any phenomena or patterns that may not have been described in previous literature.38 The analysis was conducted using tables and graphs to triangulate the relation among various combinations of variables. The goal with this type of analysis is to summarize data, describe patterns, and point toward possible causal mechanisms in a meaningful display that is helpful to the reader. The conclusions drawn from our analysis are not intended to establish causal relationships but rather to examine important dynamics between the coded variables, understand gaps in practice, and promote safe use of alteplase and tenecteplase to treat AIS.
Results II
Based on Methods II, we identified 92 event reports (alteplase n=48; tenecteplase n=44) that met inclusion criteria for Part II of our study. These 92 reports are a subset of the sample from Part I of the study.
Demographics
A total of 52 Pennsylvania hospitals submitted at least one report describing an event that was included in our study. Of these, 31 hospitals submitted one report (60%, 31 of 52), 10 hospitals submitted two reports (19%; 10 of 52), and 11 hospitals submitted three or more reports (21%; 11 of 52). More than half of the reports (57%, 52 of 92) were submitted by facilities with more than 300 beds. The “Emergency Department” care area group was identified as the location in majority of reports (71%, 65 of 92). Based on the 92 reports, patient age was an average of 67 years and a median of 68 years (range: 14 to 98 years, 25th percentile: 55 years, 75th percentile: 81 years).
Medication
As shown in Figure 3, 52% of the reports involved alteplase (48 of 92) and 48% involved tenecteplase (44 of 92) as the intended medication for AIS. Of the total reports, near misses accounted for 42% (39 of 92) and occurred with an almost equal distribution between the two medications (alteplase 51%, 20 of 39; tenecteplase 49%, 19 of 39). An event attributed to a wrong indication was described in six reports; in five tenecteplase-related events, the indication was confused for AMI, and in one alteplase-related event, the order was incorrectly placed for PE.
.jpeg)
Stage of the Medication-Use Process
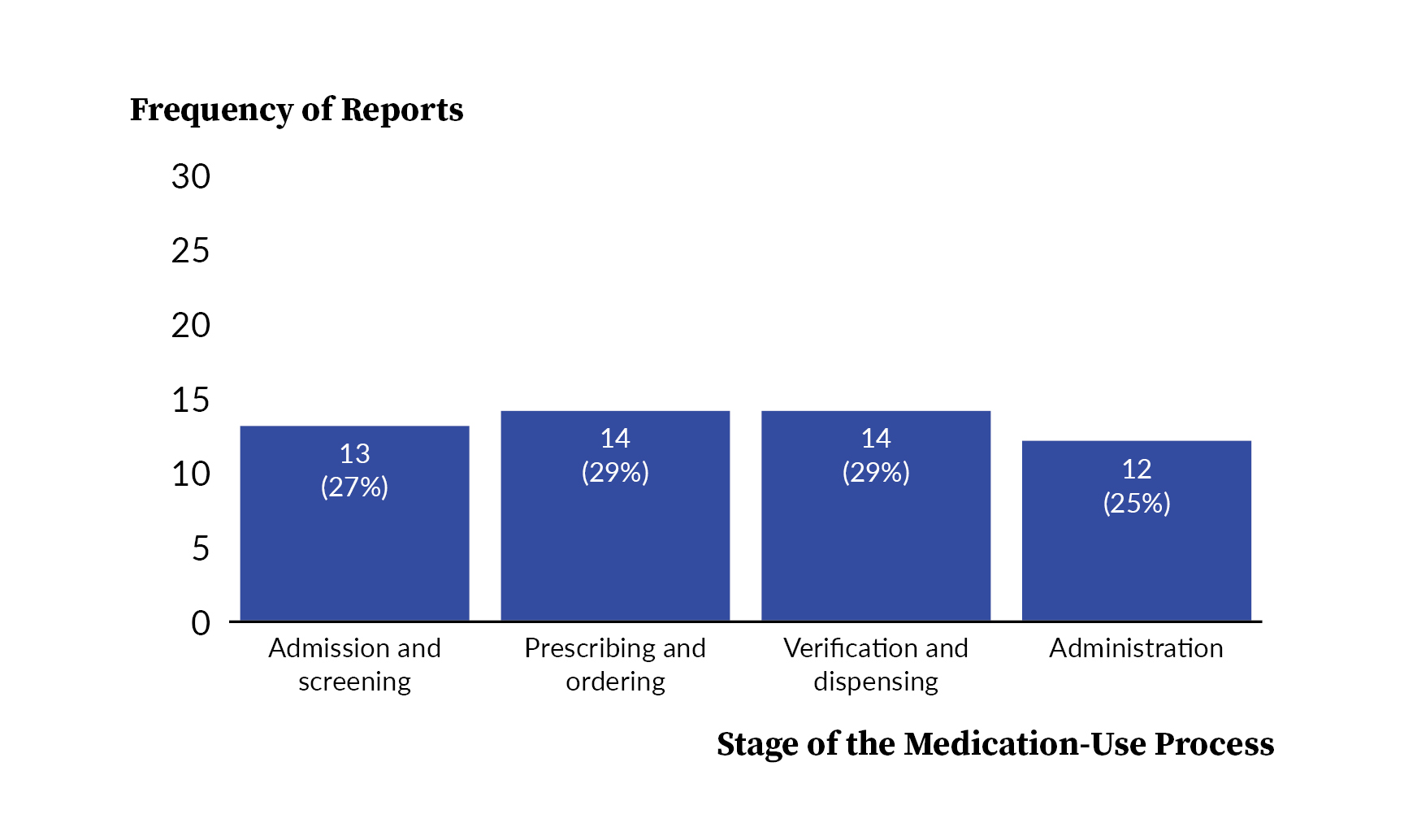
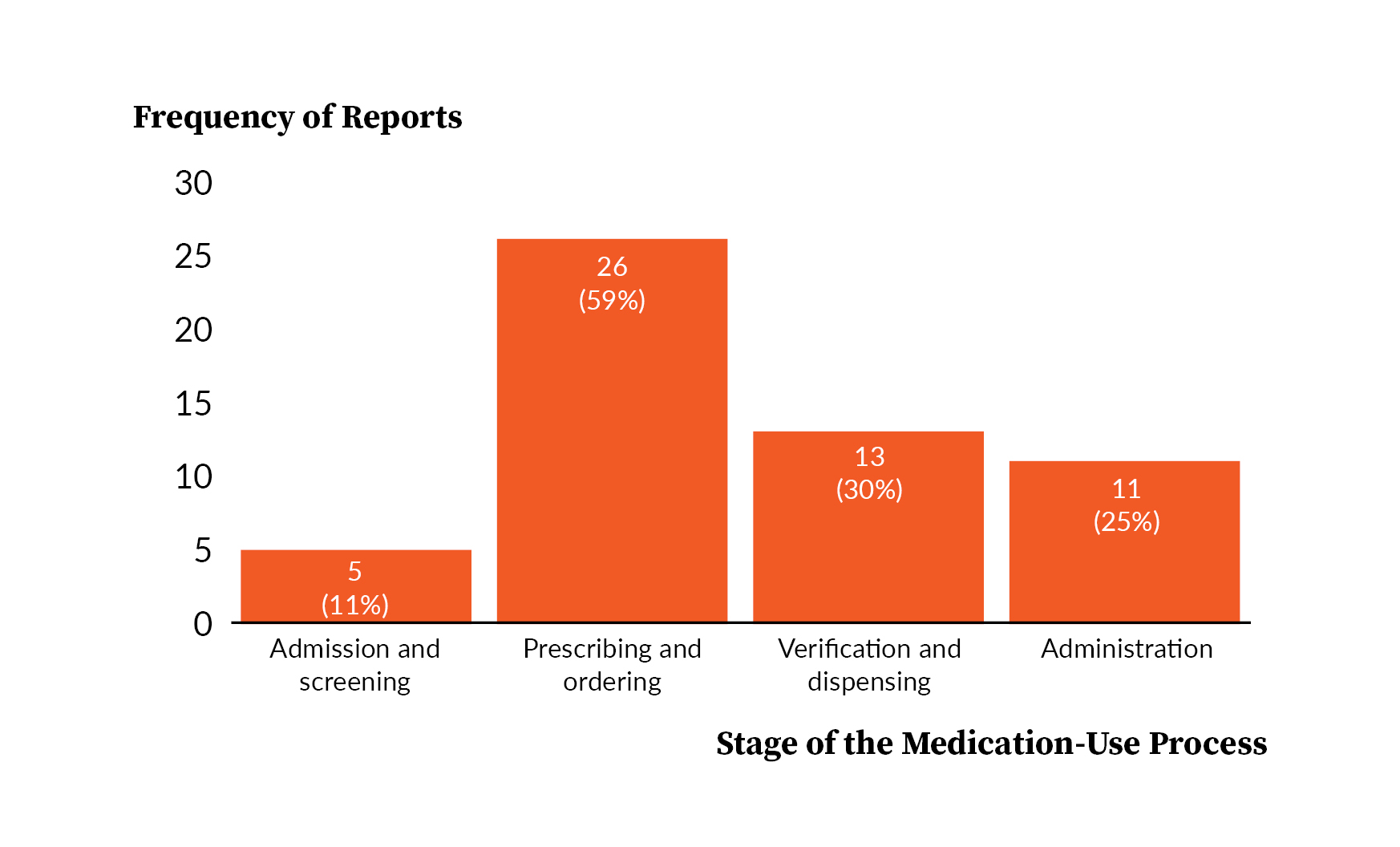
Figure 4 and Figure 5 show the distribution of each stage of the medication-use process involved by intended medication. Alteplase-related events occurred with a more similar frequency across the four stages (range of 12 to 14 reports), while the frequency of tenecteplase-related events was highly variable across the four stages (range of 5 to 26 reports). Across both medications, the Prescribing and ordering stage was associated with the highest frequency of total events (40 of 92 reports).


Associated Factor and Stage of the Medication-Use Process
Table 4 shows the frequency of associated factors by stage and intended medication. Associated factors were not mutually exclusive, resulting in a total of 120 associated factors that were coded across 92 reports. Seventy-four percent (68 of 92) of reports had one associated factor, 22% (20 of 92) had two associated factors, and 4% (4 of 92) had three associated factors coded. The associated factors we identified most frequently across all reports were Weight incorrect or not collected (13%, 15 of 120) and Order not placed in EHR (9%, 11 of 120). Knowledge and/or experience deficit, when combined across all stages of the medication-use process, was also coded frequently (10%, 12 of 120).
.jpeg)
Admission and Screening
Across all associated factors, 16% (19 of 120) occurred during Admission and screening. The associated factor Weight incorrect or not collected accounted for 79% (15 of 19) of all associated factors coded for this stage and was identified much more frequently in events involving alteplase (alteplase n=11; tenecteplase n=4).
Prescribing and Ordering
Across all associated factors, 40% (48 of 120) occurred during Prescribing and ordering. The two associated factors that were identified most frequently during this stage were Order not placed in EHR (23%, 11 of 48), which was seen more frequently with tenecteplase (alteplase n=2; tenecteplase n=9), and Order unclear or ambiguous (17%, 8 of 48), which also occurred more frequently with tenecteplase (alteplase n=3; tenecteplase n=5). Overall, two-thirds of all associated factors related to this stage involved tenecteplase (67%, 32 of 48).
Verification and Dispensing
Across all associated factors, 25% (30 of 120) occurred during Verification and dispensing. The associated factor that occurred most frequently during this stage was Dosing information unavailable or incorrect (20%; 6 of 30), which was relevant to only tenecteplase (alteplase n=0; tenecteplase n=6). Conversely, associated factors that were unique to only alteplase during this stage were Drug label wrong or missing (alteplase n=4; tenecteplase n=0) and Calculation error (alteplase n=2; tenecteplase n=0).
Administration
Across all associated factors, 19% (23 of 120) occurred during Administration. The most frequent associated factors identified for this stage were Medication administration not documented in MAR (26%; 6 of 23), Programming error with infusion pump (26%; 6 of 23), and Other (26%; 6 of 23). Tenecteplase was more frequently involved with the associated factors Medication administration not documented in MAR (alteplase n=1; tenecteplase n=5) and Knowledge and/or experience deficit (alteplase n=1; tenecteplase n=4), while Programming errors with infusion pump was relevant to only alteplase (alteplase n=6, tenecteplase n=0). The alteplase-related events coded as Other, Administration consisted of the inappropriate administration of infusion prior to bolus, bolus pushed too fast, suboptimal connection of lines preventing drug administration, and wrong manipulation of the infusion bag leading to drug waste.
Event Type
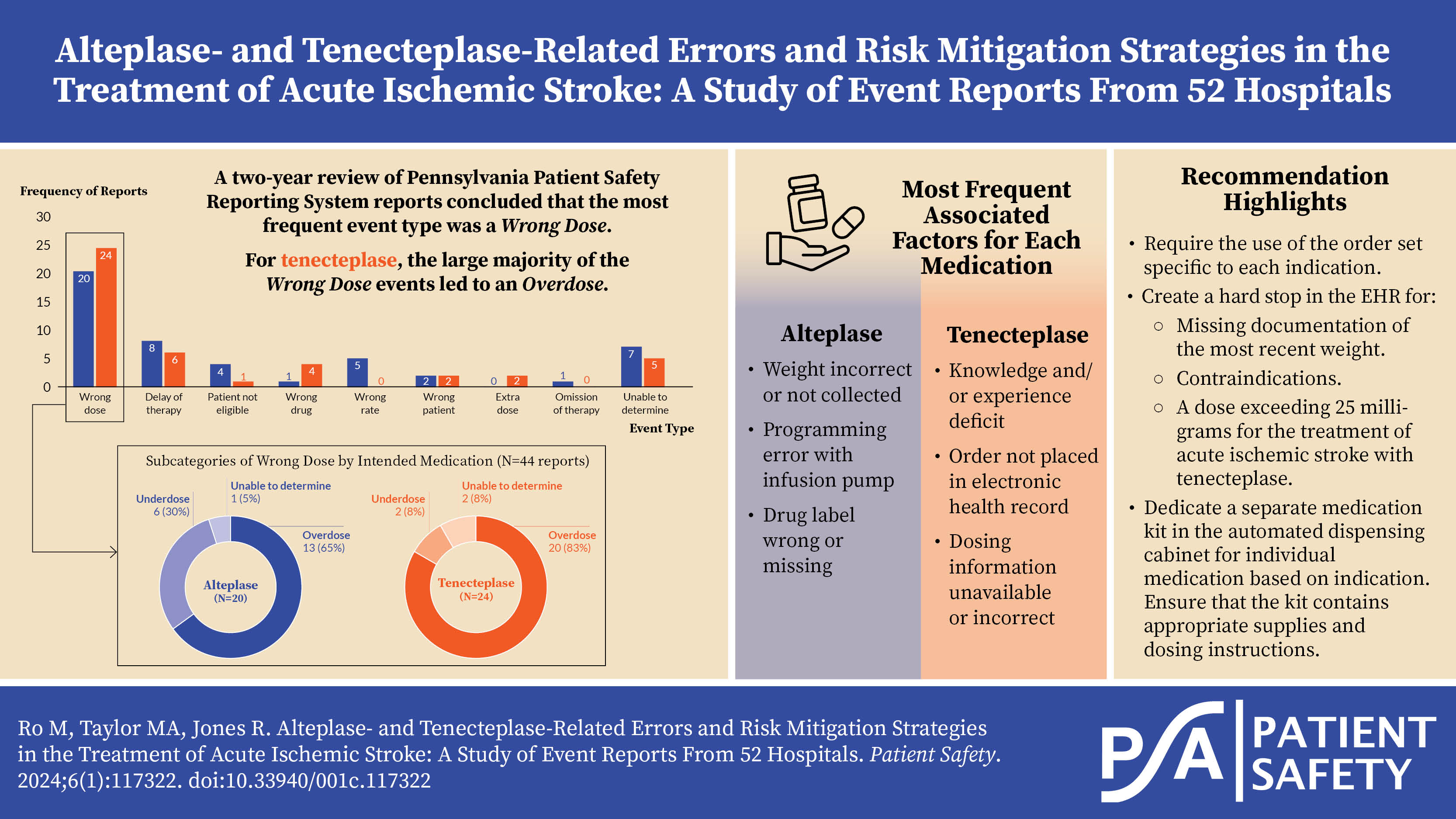
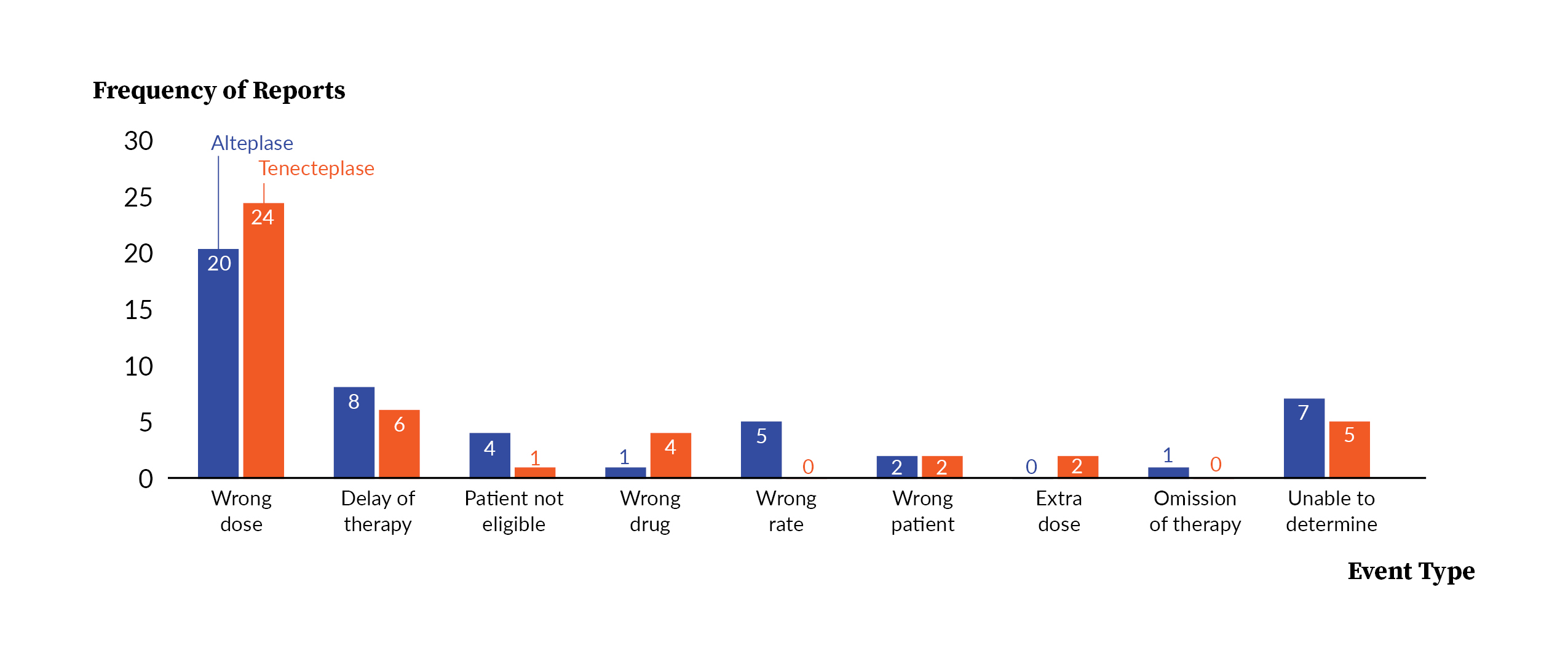
Figure 6 shows the distribution of event types by intended medication. Based on a total of 92 reports, the event types we identified most frequently were Wrong dose at 48% (44 of 92) and Delay of therapy at 15% (14 of 92). The event type Wrong rate was unique to alteplase only (alteplase n=5; tenecteplase n=0), and several event types occurred more frequently for tenecteplase, such as Wrong drug (alteplase n=1; tenecteplase n=4).
.jpeg)
Figure 7 shows the subcategories of Wrong dose for each medication: Overdose, Underdose, and Unable to determine. Collectively, 75% (33 of 44) of all reports coded as Wrong dose resulted in an overdose. Among these, tenecteplase accounted for the majority of events leading to an overdose (alteplase n=13; tenecteplase n=20).
.jpeg)
Event Type, Stage, And Associated Factor
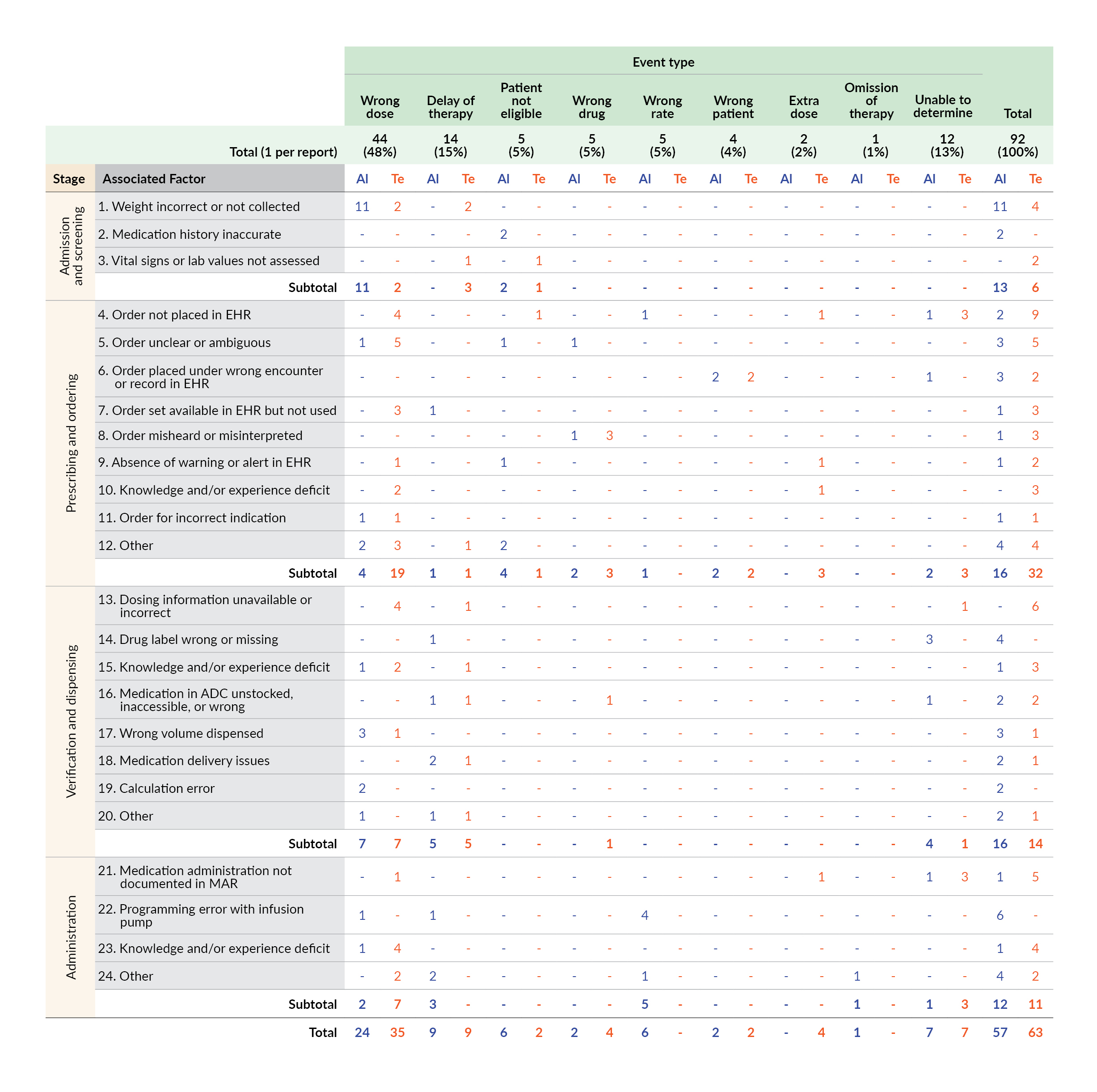
Table 5 shows the frequency of stages, associated factors, and event types for each of the intended medications. The distribution of the event type Wrong dose and corresponding associated factors by stages are described further in the next section. The event type Delay of therapy had the second highest frequency of associated factors (alteplase n=9; tenecteplase n=9), and more than half of these associated factors occurred during the Verification and dispensing stage (56%; 10 of 18).
__stages__and_associated_factors_(n_12.jpeg)
The event type Wrong drug was detected more frequently with tenecteplase and could be attributed primarily to the associated factor Order misheard or misinterpreted (alteplase n=1; tenecteplase n=3). In fact, all events that had the associated factor Order misheard or misinterpreted involved the use of the abbreviation “TPA” and led to the event type Wrong drug.
The event type Wrong rate was relevant to only alteplase, was mostly impacted by the Programming error with infusion pump associated factor (4 of 6), and was related with only two stages of the medication-use process: Prescribing and ordering and Administration.
The associated factor Order not placed in EHR was identified more frequently for tenecteplase (alteplase n=2; tenecteplase n=9) and resulted in the most diverse distribution of event types, which signifies that missing or undocumented orders can lead to many different types of events.
Wrong Dose and Associated Factor
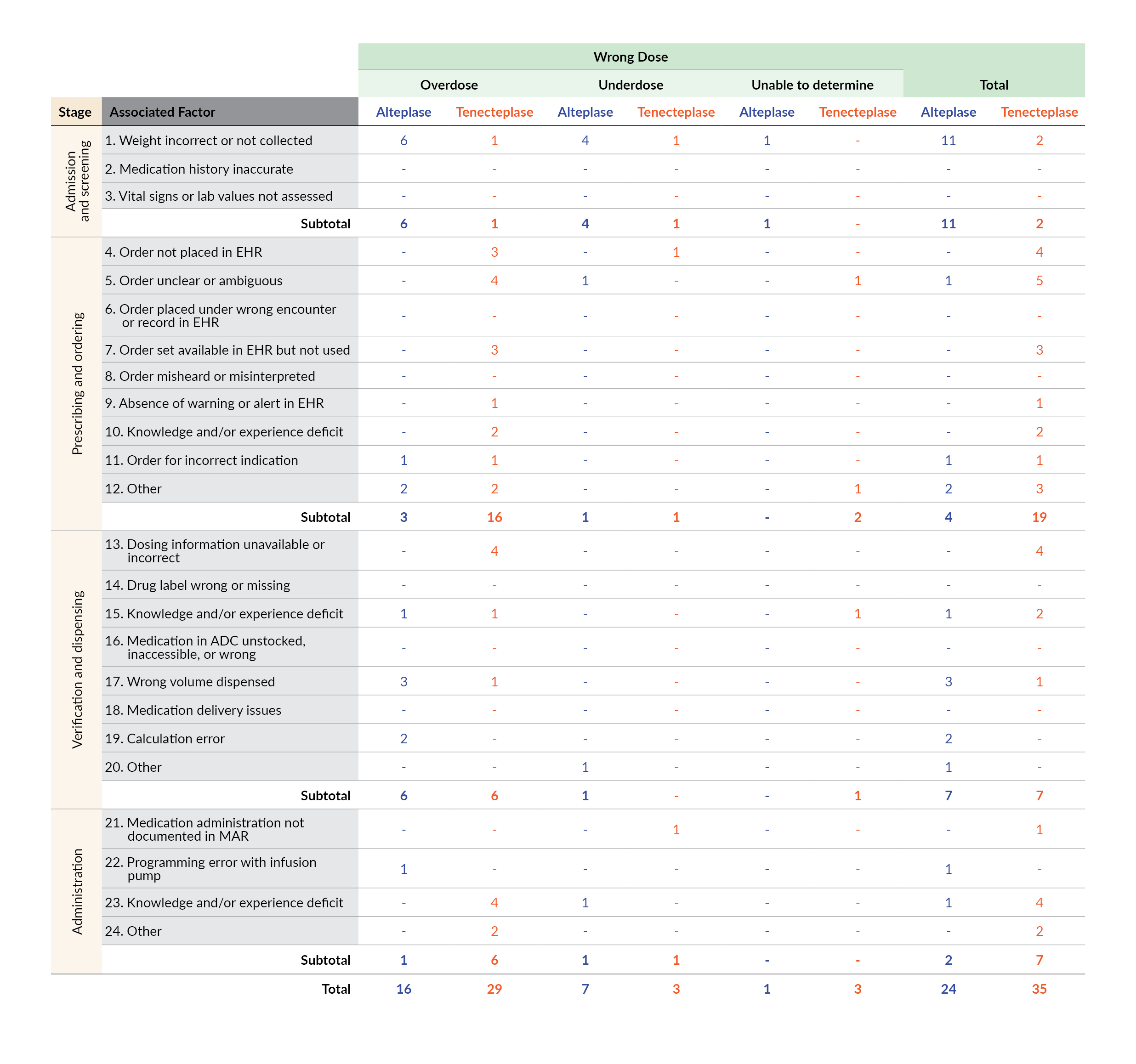
The complete table of associated factors for the event type Wrong dose, as detailed by Overdose, Underdose, and Unable to determine, can be found in Table 6. An overdose involving alteplase was most frequently associated with Weight incorrect or not collected (n=6), Wrong volume dispensed (n=3), and Calculation error (n=2). Two of these categories of associated factors, Wrong volume dispensed and Calculation error, both involved the wrong dose preparation during the Verification and dispensing stage as a result of the failure to remove the correct amount of overfill and/or incorrect calculation of bolus and/or infusion doses.
_by_subcategories_of_*wrong_dose*_(n_44)_and_intended.jpeg)
For tenecteplase, overdoses were most frequently related with the associated factors Knowledge and/or experience deficit (n=7), Dosing information unavailable or incorrect (n=4), and Order unclear or ambiguous (n=4). The associated factor Knowledge and/or experience deficit spanned across three different stages, Prescribing and ordering, Verification and dispensing, and Administration, which highlights the prevalence and implication throughout the medication-use process. All four reports coded with the associated factor Dosing information unavailable or incorrect involved confusion with the wrong indication for AMI, which led to exceeding the maximum dose of 25 milligrams recommended for the treatment of AIS.
A quarter of all tenecteplase-related overdose events (25%; 5 of 20) involved a wrong indication in which a staff member either chose a wrong order set intended for AMI in the EHR or followed the wrong dosing instructions intended for AMI provided in the medication kit.
Discussion
In Part I of our study, we measured the frequency of reports submitted to PA-PSRS in which either alteplase or tenecteplase was the medication prescribed, regardless of indication, and this revealed a notable increase in reported events involving tenecteplase. In Part II of our study, we analyzed numerous variables to better understand the nature of medication errors involving the use of either alteplase or tenecteplase to treat AIS. To our knowledge, this is the first study of medication events involving alteplase and tenecteplase to treat AIS that delineated event types and associated factors with the stage of the medication-use process.
For both medications, we found Wrong dose to be the event type with the highest frequency, which was identified in almost half of all reports included in the study. For alteplase, Weight incorrect or not collected was the factor most frequently associated with Wrong dose. When an inaccurate weight is used to calculate the dose, the patient could receive a dose that is considerably different from what is appropriate, safe, and effective.39 For example, two separate studies of reports found that 44% and 42% of all wrong weight events led to an overdose.39,40 In our study, the associated factor Weight incorrect or not collected was identified in 55% of all events that were coded overdoses with alteplase.
Additionally, we found that the Verification and dispensing stage and Administration stage of the medication-use process were associated with several safety gaps unique to alteplase. Our findings revealed safety challenges associated with the multistep preparation of the bolus and infusion doses of alteplase, use of the infusion pump, and different rates of administration for bolus and infusion. For example, we identified the associated factor Programming error with infusion pump and the event type Wrong rate only in reports involving alteplase.
Unlike alteplase, the bolus administration of tenecteplase eliminates problems associated with use of an infusion pump, such as setup issues, air in tubing, and staff required during interfacility patient transfers.10,11 It has also been shown to be associated with a shorter door-to-needle time.8,32
Despite these advantages, our study showed that tenecteplase has several distinct safety gaps. Many were related to the use of a medication kit and confusion with a wrong indication (AMI) leading to an overdose. Because tenecteplase is currently approved for the treatment of AMI only, the medication is supplied from the manufacturer inside a kit that contains dosing, preparation, and administration instructions intended for AMI, not AIS.4,41 The maximum recommended dose of tenecteplase for treatment of AMI as provided in the kit is 50 mg, which is double the maximum recommended dose of tenecteplase for the off-label treatment of AIS.4,18,41 Accordingly, in our study, all tenecteplase-related events coded as Dosing information unavailable or incorrect led to the event type Wrong dose and were in fact, overdoses.
Furthermore, more than half of the reports involving tenecteplase involved the Prescribing and ordering stage of the medication-use process. In particular, several associated factors involving the use of the EHR were identified more frequently with tenecteplase than with alteplase, such as Order not placed in EHR, Order set available in EHR but not used, and Absence of warning or alert in EHR. During the Administration stage, the associated factor Medication administration not documented in MAR was also identified more frequently with tenecteplase. These findings suggest that providers are not using the EHR to place or document an order, orders are placed without using the correct order set, and the EHR is not optimized to detect and mitigate errant orders.
Lastly, the associated factor Knowledge and/or experience deficit was identified across multiple stages, occurring throughout Prescribing and ordering, Verification and dispensing, and Administration stages. When combined altogether across the stages, it represented the second most frequently coded associated factor in the study, and 83% of these were observed with tenecteplase. This indicates that the lack of knowledge and/or experience with tenecteplase was a factor in many events.
Potential Strategies
Table 7 shows a list of potential strategies that can be adopted at the provider and system levels. Because every facility has its own unique workflow, processes, and resources, it is important to identify those that are both applicable and meaningful to each facility. The potential strategies should be reviewed with the interdisciplinary members of the stroke team and the relevant hospital committees, as well as the patient safety officer and the medication safety officer of the institution, with the overall goal of assessing current practices and continuously monitoring for improvement.

Limitations
One limitation of our study is the inherent nature of event reporting; a report does not necessarily represent the results of a thorough investigation and therefore may not provide insight into root causes. We do not recommend using our results for benchmarking or direct comparison because differences in culture, patient populations, resources, and error detection methods and systems may exist across facilities.57 In addition, the definitions used in our study may differ from definitions used in other studies. For example, one study involving alteplase defined “delay” as a contributing factor,37 while our study described it as an event type. Other studies may also categorize the medication-use process into stages different from those in our study.58 Readers are encouraged to carefully compare results from other similar studies and refer to Methods II for definitions used in our study.
Given that this study presents aggregate data, facilities may gain important insight from performing site-specific investigations, such as a root cause analysis to retrospectively examine an event, a medication-use evaluation (MUE)59,60 to answer a particular safety question, or a failure mode and effects analysis (FMEA)49,50 to prospectively identify and mitigate high risk processes.
Conclusions
Both alteplase and tenecteplase have been used in clinical practice for decades; however, the increasing off-label use of tenecteplase for the treatment of AIS5,7,8,11,61,62 created new safety challenges. By analyzing the stages of the medication-use process, associated factors, and event types, we identified aspects to medication safety that occurred with both alteplase and tenecteplase, as well as those that were unique to each individual medication. The event type Wrong dose was the most prevalent event type for both medications; however, the related stages and associated factors for the individual medication were variable. Our study underscores the need for increased awareness surrounding these medication errors and the provision of necessary support and training for providers. We encourage readers to review the potential strategies that fit the needs of their institutions and to supplement the analyses of their own institution-specific data and investigations with our findings to improve safety of patients receiving thrombolytics for treatment of AIS.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
Myungsun (Sunny) Ro (mro@pa.gov) is a research scientist on the Data Science & Research team at the Patient Safety Authority (PSA). Her responsibilities include analyzing and synthesizing data from various sources to identify opportunities to improve patient safety, as well as writing scientific articles for publication in the PSA’s peer-reviewed journal, Patient Safety.
Matthew A. Taylor is a research scientist on the Data Science & Research team at the Patient Safety Authority (PSA), where he conducts research, uses data to identify patient safety concerns and trends, and develops solutions to prevent recurrence. He is a core team member of PSA’s Center of Excellence for Improving Diagnosis.
Rebecca Jones is director of Data Science & Research at the Patient Safety Authority (PSA) and founder and director of the PSA’s Center of Excellence for Improving Diagnosis.
PA-PSRS is a secure, web-based system through which Pennsylvania hospitals, ambulatory surgical facilities, abortion facilities, and birthing centers submit reports of patient safety–related incidents and serious events in accordance with mandatory reporting laws outlined in the Medical Care Availability and Reduction of Error (MCARE) Act (Act 13 of 2002).34 All reports submitted through PA-PSRS are confidential and no information about individual facilities or providers is made public.
This criterion was verified through manual review of the event narrative in the report.
This criterion was verified through manual review of the event narrative in the report.
Within the PA-PSRS acute care database, there are 168 care areas for facilities to use to identify where events occur. Each of these care areas is then placed into one of 23 higher level care area groups.