
Introduction
Building a culture of accountability and transparency in healthcare can be challenging. Employees should feel confident that reporting medication errors will result in system improvements for patient care. This type of cultural transformation takes time for an organization to achieve. The Committee on Identifying and Preventing Medication Errors, commissioned by the Institute of Medicine (now the National Academy of Medicine), estimated that every hospital patient experienced at least one medication error each day.1 Drugs in the medication class neuromuscular blocking agents (NMBAs) have been identified as medications that have been given in error to hospitalized patients, often causing significant harm.2 A 2009 study published by the Patient Safety Authority identified 154 incidents with NMBAs reported over a five-year period. Thirty-seven percent of those errors within this drug class involved the use of the wrong medication.3 A tragic and highly publicized medication error involving an NMBA resulted in a patient’s death at a large academic medical center (AMC) in December 2017.4
NMBAs are indicated as high-alert medications (HAMs) according to the Institute for Safe Medication Practices (ISMP) and demand special handling due to a heightened risk of patient harm.5 These medications temporarily paralyze the muscles and are most frequently used when a patient has a protected airway and is intubated. An overdose of this agent or use of the drugs when a patient does not have a protected airway results in decreased respiratory drive and respiratory failure.6 In December 2017 at a large AMC, a nurse mistakenly administered intravenous (IV) vecuronium, a neuromuscular blocking agent, instead of Versed (midazolam), an anxiolytic drug, to a radiology patient. Of note, the brand name of midazolam, Versed, has been discontinued in the United States as of 2003.7
As a “help-all” nurse, a role not formally recognized in the literature, they often assisted other nurses with patient care tasks. On this occasion, they were assigned to administer IV Versed to a patient because the radiology nurse felt uncomfortable doing so. They typed “ve” into the automated dispensing cabinet (ADC) to retrieve the medication, but “Versed” was not found since the default search within the ADC was generic name only. When they failed to locate it, they overrode the list of medications approved for patient use in the cabinet, which allowed for a search by brand or generic name. They then selected the first medication that had “ve” in its name, which happened to be vecuronium.
Normally, overrides occur for urgent or emergent situations prior to a pharmacist reviewing the order; however, in this scenario, the override appears to have been routinely used by staff at the facility. The patient was given vecuronium instead of midazolam and ultimately passed away as a result. This fatal medication error ultimately resulted in the nurse’s termination at AMC, underscoring the lack of a “just culture.” Furthermore, their nursing license was indefinitely revoked, accompanied by additional fines. Following a jury trial in 2022, they were found guilty and charged with criminally negligent homicide and abuse of an impaired adult.8
Following the error, the Centers for Medicare & Medicaid Services (CMS) completed an unannounced site visit between October 31 and November 8, 2018. Succeeding the visit, CMS issued a report to AMC regarding deficiencies in care and required a corrective action plan from the organization to prevent such errors from recurring. The document containing the CMS statement of deficiencies and AMC’s plan of correction are publicly available.9 Our analysis of the AMC’s corrective action plan was contrasted with ISMP’s hierarchy of effectiveness of risk-reduction strategies to determine the strength of reported interventions against a published standard. The purpose of the analysis was to provide a framework for developing future corrective action plans following fatal medication errors that might occur in healthcare facilities.
The strongest interventions are those from the top level of ISMP’s hierarchy of effectiveness which embody system reliability over human reliability.
According to ISMP’s reporting on AMC’s event and the nurse’s subsequent trial, the defense counsel did not educate the jury on how system failures or flaws in the medication-use process contributed to the error that occurred. Such an omission was likely a contributing factor to the criminal sanctions that they faced.10 This could have harsh implications for future patient safety cases because implementing ramifications to individuals discourages medication error reporting, thus preventing a systemic issue from being fixed. Although the case has received significant attention from the press and the healthcare community, there may still be underlying issues to be addressed. The consensus among all involved is that the situation should not recur and that the error was preventable.
Analysis of AMC’s Corrective Action Plan as It Fits Into ISMP’s Hierarchy of Effectiveness
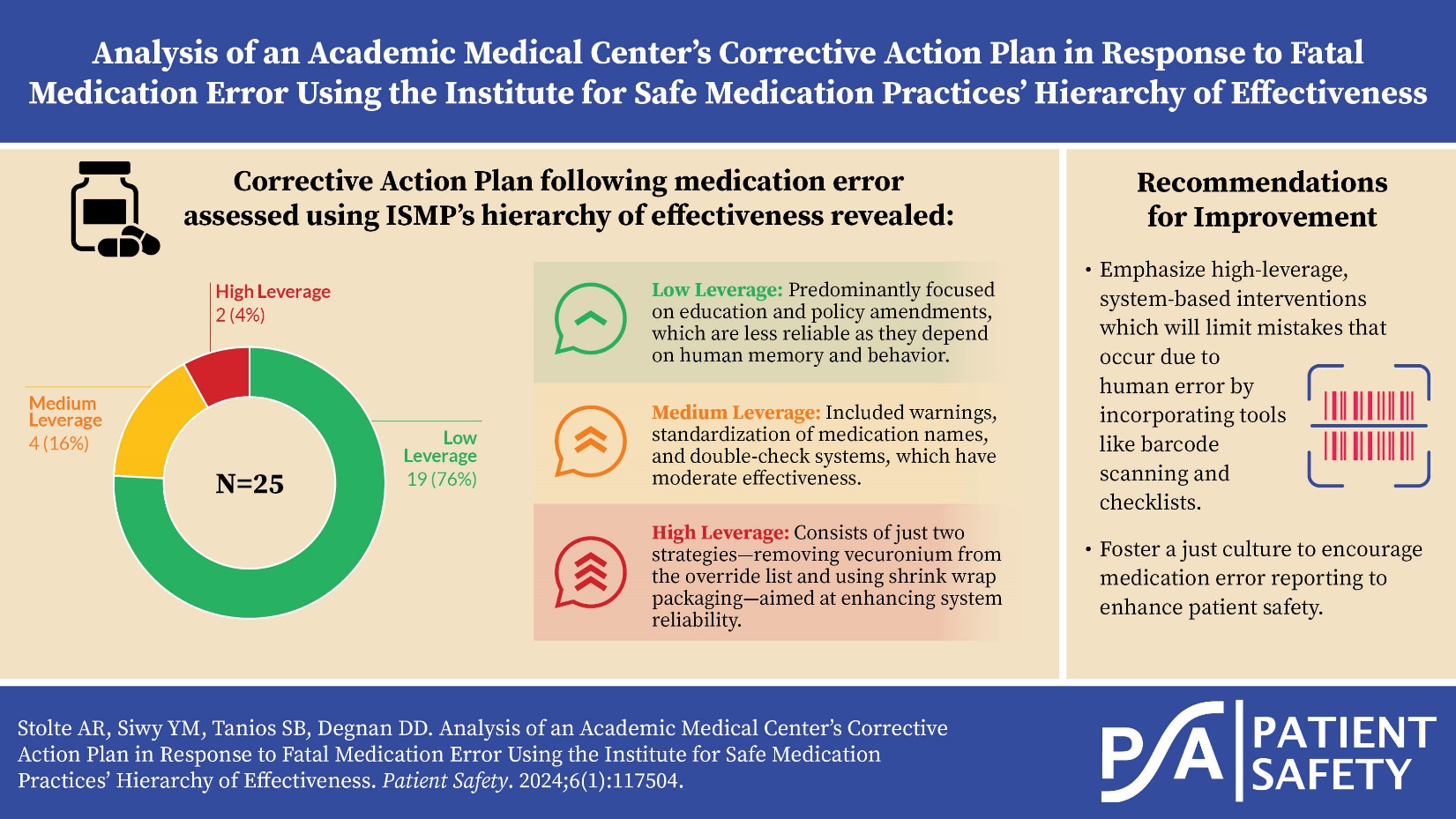
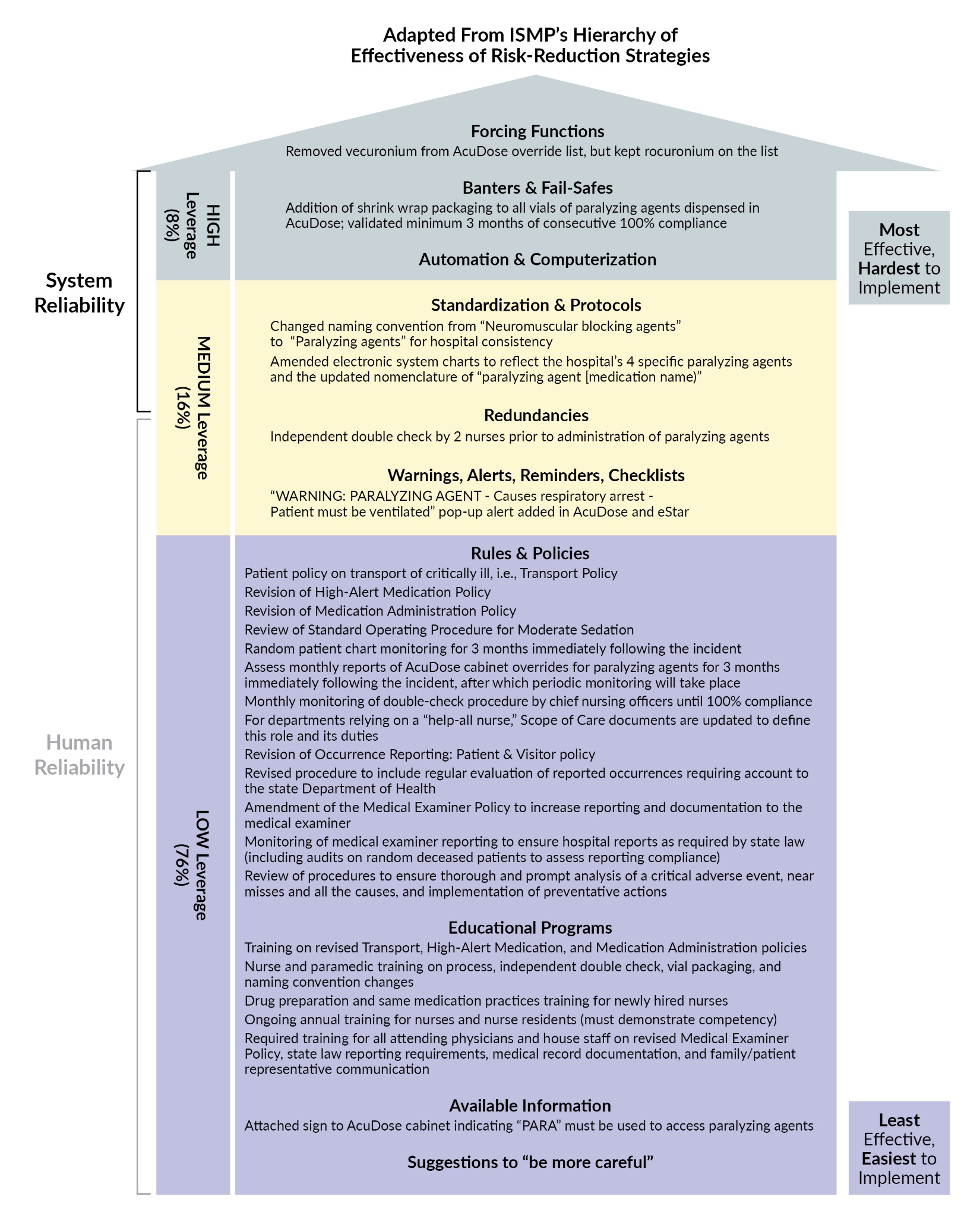
The ISMP hierarchy of effectiveness is a framework for preventing errors and improving patient safety in healthcare. The hierarchy ranks interventions based on their effectiveness in reducing errors and harm.11 The authors of this paper reviewed AMC’s corrective action plan, classifying its components and assessing their alignment with ISMP’s hierarchy. Notably, this is the only analysis to thoroughly assess this corrective action plan against a nationally recognized hierarchy. As displayed in Figure 1, of the 25 implemented strategies, two were classified as high leverage (8%), four were classified as medium leverage (16%), and the remaining 19 were classified as low leverage (76%).

More than 75% of these strategies focused on education and policy amendments. According to ISMP and other references, education is frequently identified as one of the least effective correction strategies because it relies on human memory and behavior, rendering it often unreliable in preventing errors.11 These limitations stem from understaffing, miscommunication, disruptions, shortcomings in safety culture, and external stressors, all of which can contribute to medication errors.12 In addition, amending policy language can be ineffective in preventing error because doing so frequently adds complexity or provides vague or untenable direction to staff. There can also be gaps when translating written policies into practical actions due to miscommunication or workplace conditions.13 When implemented alone, education and policy revisions are often the least effective interventions when attempting to prevent an error from recurring.
Of AMC’s corrective action plan strategies, 16% fell into the medium-leverage category, including interventions related to warnings, standardization of medication names, and a double-check system. While warnings are important for high-alert medications, the potential for alert fatigue over time may lead to overrides or disregard of warnings.14 In addition, the implementation of a two-nurse double-check system for paralyzing agents may help identify near misses, but standardization of the checking process is necessary to minimize process variations.15 In this case, however, the nurse assumed they had Versed, not vecuronium, so they would not have requested a double check. To enhance safety measures, the corrective action plan should address the system for anxiolytics like Versed. However, implementing a double-check system for every medication prone to confusion with paralyzing agents might lead to oversaturation and render the strategy ineffective. The more effective strategy involved updating the nomenclature in the electronic systems at AMC to reflect the classification of the high-risk paralyzing agent, helping to standardize the process of its dispensing. Nurses are now required to input “PARA” to access the medication, which limits options to paralyzing agents only.
Only two of the 25 strategies (8%) identified by AMC fell within the high-leverage category and exhibited systems-based reliance. Of the two, one is purported to have higher effectiveness according to ISMP. The less-effective approach involved using shrink wrap for all paralyzing agents to prevent confusion with other medications. However, it is categorized in a lower tier because it relies on man-made barriers and cannot ensure a completely fail-safe environment. The strategy of removing vecuronium from the override list is more effective by reducing access to the medication; however, it’s worth noting that other NMBAs, such as rocuronium, were not included.
Effective Strategies to Prevent Medication Errors in Healthcare
Based on a comparison of AMC’s corrective action plan to ISMP’s hierarchy of effectiveness, a continued focus on high-leverage strategies to prevent errors across healthcare is necessary. While there’s no quantitative data affirming the probable failure of AMC’s corrective plan, the inevitability of human error highlights the necessity for robust interventions. The strongest interventions are those from the top level of ISMP’s hierarchy of effectiveness which embody system reliability over human reliability. Examples of these types of interventions include removing injectable potassium chloride from all patient care areas (forcing function) and computerized physician order entry with clinical decision support to standardize the order process and inherently account for drug interactions and allergies (automation and computerization), the latter of which applies to both inpatient and outpatient care models.13,16
However, AMC’s corrective action plan appears to lack interventions aligned with ISMP’s Targeted Medication Safety Best Practices for Hospitals for paralyzing agents.17 These practices advocate for actions such as eliminating unnecessary storage of NMBAs, restricting access to essential areas within rapid sequence intubation (RSI) kits, segregating NMBAs from other medications, affixing auxiliary labels on all NMBA storage containers, and implementing ADC alerts mandating clinical information before dispensing.17 Incorporating such interventions could fortify medication safety protocols within AMC’s corrective strategy.
By fostering a just culture, acknowledging the inevitability of human fallibility, and nearly eliminating human reliability, there exists the potential to revolutionize patient safety.
A systems-based intervention listed as “pending” in the corrective action plan was the use of barcode technology at medication administration. Barcode scanning not only helps meet the goal of the five rights of medication administration (right drug/dose/time/route/patient), but it also decreases the rate of adverse drug events (ADEs) by about 20%.18 Barcode scanning to compare the paralytic agent, the patient’s wristband, and the patient’s medication order may have prevented this tragedy. Based on the corrective action plan, it is not clear if the use of barcode technology was implemented in radiology, although others have reported that it has been.19 A tool not mentioned in the corrective action plan was the use of checklists. A checklist for caregivers administering high-alert medications or a medication outside of the normal scope of practice can improve the reliability and standardization of a process, particularly checklists that are highly specific and detailed.15 Both barcode technology and checklists are examples of safety tools that provide process-based solutions rather than relying on human performance.
The Role of Just Culture
Preventing future medication errors requires more than only system changes. A crucial contributing factor in this tragedy was the absence of a “just culture,” which refers to "a system of shared accountability in which organizations are accountable for the systems they have designed and for responding to the behaviors of their employees in a fair and just manner.20 AMC’s decision to terminate the nurse highlights the absence of a just culture in this scenario. When organizations solely blame individuals, it discourages error reporting, hindering the necessary corrections to the system. By fostering a just culture, acknowledging the inevitability of human fallibility, and nearly eliminating human reliability, there exists the potential to revolutionize patient safety.
Conclusion
A comparison of AMC’s corrective action plan following a fatal medication error in 2017 to ISMP’s hierarchy of effectiveness demonstrated minimal use of high-leverage interventions. The error at AMC should not be regarded as a testament to human fallibility; rather, it accentuates the burden placed on people to achieve perfect outcomes within a system that inherently relies on human perfectionism, an unrealistic expectation. The inherent complexity and error-prone nature of the medication-use process necessitates a shift from individual blame to a recognition of systemic challenges. Embracing a just culture and prioritizing system reliance over human perfectionism are vital steps in enhancing patient safety. Moving forward, corrective action plans must adopt a systems-based approach, subject to rigorous evaluation by CMS. Mitigation strategies should emphasize high-leverage interventions to address human fallibility effectively. Beyond the realm of NMBAs, the objective remains to build resilient and robust medication systems to prevent such errors.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
Aubrey R. Stolte (stolteaub99@gmail.com) is a PharmD candidate at Purdue University College of Pharmacy.
Yasmin M. Siwy is a PharmD candidate at Purdue University College of Pharmacy.
Sarah B. Tanios is a current Regulatory Pharmaceutical Medication Safety Fellow with Purdue University, AbbVie, and the Food and Drug Administration.
Daniel D. Degnan is a courtesy clinical assistant professor at Purdue University College of Pharmacy.