



Introduction
Smart infusion pumps with dose-error reduction software (DERS) and customizable drug libraries have increased the safety of intravenous (IV) infusion delivery.1,2 Smart pumps allow organizations to create, edit, and maintain drug libraries with dose, duration, and concentration limits to alert clinicians when parameters are programmed outside of the facility-accepted ranges.
Routine update of the drug library is recommended.3,4 The Institute for Safe Medication Practices endorses at least quarterly drug library updates to incorporate new drug information, formulary and practice changes, and quality improvement data.5 Furthermore, maintaining the most up-to-date drug library on an organization’s fleet of smart pumps reduces potential harmful events such as false alerts and alarm fatigue associated with outdated libraries.6,7
Updating a drug library on a smart pump is an active process that requires multiple steps, from creation of the new drug library file to activation of the drug library on an individual pump. Depending on the manufacturer, the process for activating the drug library may differ. For some smart pumps, activation of the new library is not automatic; rather, it requires involvement from various participants.6
Delays in drug library activation on pumps have been reported.8 DeLaurentis et al. evaluated 12 health systems in a retrospective review of infusion pump data and found median delays in completion of the drug library update ranging from days to months.9 Additionally, Poppe and Eckel reported on a process improvement for drug library updates at an academic medical center that resulted in an 80% activation mark at 22 days after library release.
Delays in activating the drug library have also been shown to impact patient safety. Evaluation of library activation rates at one health system showed more than 50% of pumps were using outdated drug libraries and these outdated drug libraries were associated with 22.6% of alerts firing.10 The authors noted the outdated libraries can create inconsistencies for the pump users, can result in patient harm secondary to incorrect drug limit set up, and can cause confusion which could result in bypassing of the drug library altogether. At our organization, we have had similar safety events reported that were ultimately determined to be related to outdated drug libraries on the pump. Investigation into these events determined end users were unable to program pumps with new formulary additions or standard concentration changes because the pump was not updated with the new drug library.
Background
UW Health is a three-hospital system in Madison, Wisconsin, consisting of a 505-bed Level I academic medical center, a 56-bed community hospital, and a 111-bed children’s hospital. UW Health utilizes the BD Alaris (Becton, Dickinson and Company) infusion pump to deliver large-volume, syringe, and patient-controlled analgesia. UW Health has approximately 1,500 Alaris pump programming units across its system. Additionally, UW Health has implemented interoperability with its Epic electronic medical record and utilizes a network server for wireless pump library updates.
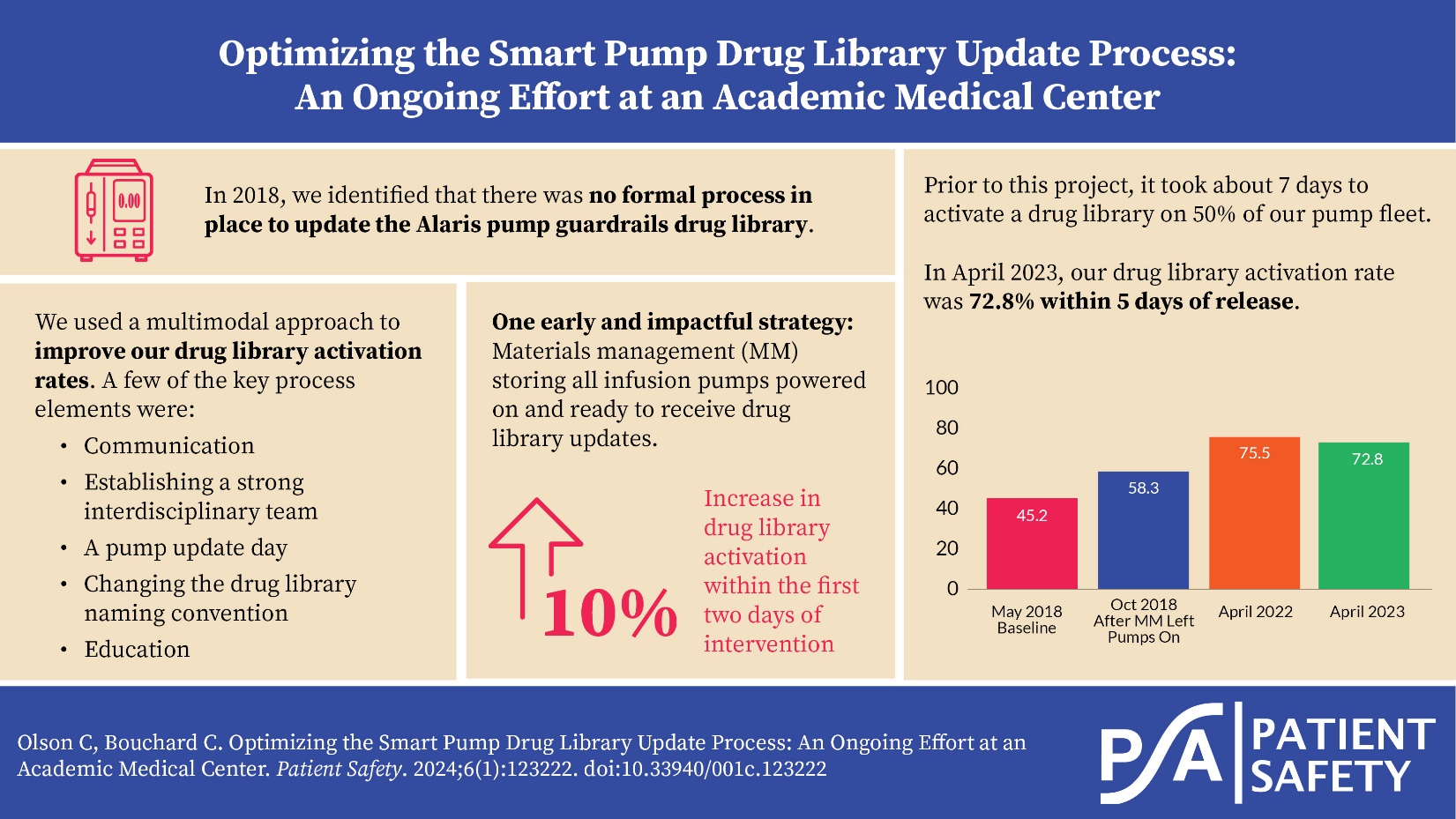
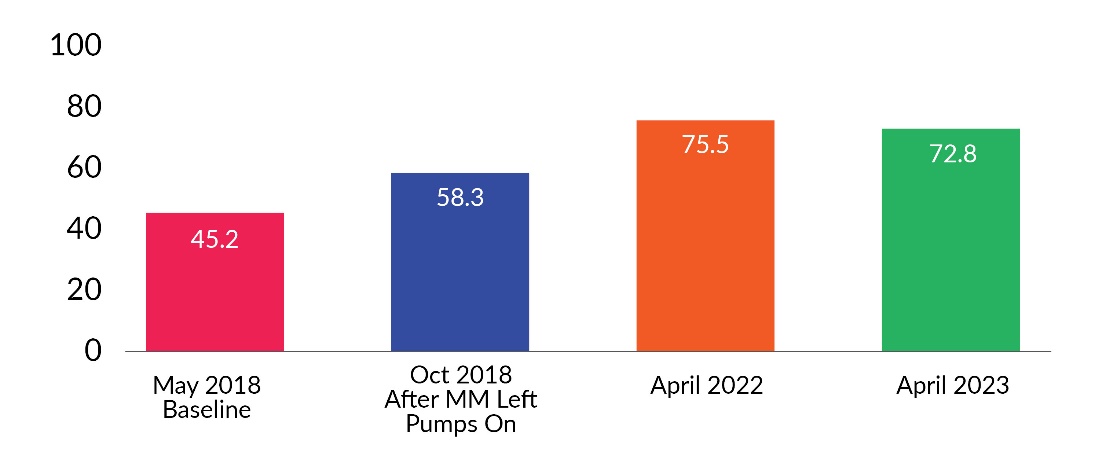
In 2018, the drug library activation statistics were evaluated as part of a quality improvement analysis associated with UW Health’s Smart Pump Oversight Committee. At that time, it took approximately seven days to activate 50% of the fleet (see Figures 5 and 6). Additionally, there were multiple versions of the drug library active on the pumps in the fleet, some dating back months prior. This was identified as a safety risk, and an evaluation of all aspects of the drug library update process was started. The goal was to identify barriers related to the drug library update process and implement changes to optimize drug library activation times.
Process
This ongoing quality improvement project began in 2018 (see Figure 1). The first step was reviewing the existing process for updating the drug library. For Alaris pumps, updating the infusion pump library starts with the release of a new drug library file to the network server. The pumps that are powered on take up the library in the background and store the library file until the pump is powered off. Once the pump is powered back on, the new library file is activated only if the pump user selects “yes” to the “new patient” prompt. For those pumps that are powered off when the library is released to the server, they must be powered back on to take up the library before completing the steps to activate the new library file.

Feedback from UW Health shared governance nursing councils, the Smart Pump Oversight Committee, and other key stakeholders demonstrated there was no standard process in place and the importance of this process was not as widely recognized as expected. Thus, it was concluded improvements in education, awareness, and follow-up were needed.
Key Process Elements
Communication. Prior to the improvement project, the only communication about the drug library update was an email sent only to inpatient clinical nurse specialists and inpatient nurse managers. This communication did not reach outpatient areas, nursing directors, pharmacy, or biomedical engineering. The content of the email acknowledged the drug library update and included the new drug library name but lacked details about the activation process or the changes included in that new library.
The changes made to the communication process entailed broadening the audience and improving the details conveyed to the clinicians. To accomplish this, communication now includes both an email and an announcement at huddles. The email is sent on the morning of the pump update and is addressed to nursing directors, nurse managers, clinical nurse specialists, nursing informatics specialists, nursing education specialists, nursing care team leaders, pharmacy, and biomedical engineering. The email content was revamped to contain the new drug library name, the details of the drug library changes for each patient care profile, and directions for how to activate the drug library on the pump. Additionally, a troubleshooting document is attached to the email to help clinicians who have difficulties activating the drug library on a pump.
The huddle communication starts at the systemwide huddle and then is shared through cascading unit huddles to the end users. The announcement at the systemwide huddle continues for the two days following the drug library update to keep this top of mind. Pump activation statistics are also shared on those days to prompt follow-up on the process.
Individual nursing units are then responsible for ensuring infusion pump drug libraries are activated. Many units have implemented a process to sign off the rooms that pumps are being used in when the pump library is activated. This sign-off is kept at the nurses’ station until all rooms and pumps are signed off.
Keeping Infusion Pumps Powered in Materials Management Area. Because the infusion pumps need to be powered on to take up the new drug library file, a go-and-see was completed to evaluate the circulation pathway of pumps from reprocessing to the patient care units. It was noticed that after the infusion pumps passed through reprocessing, they were taken to the materials management (MM) area where they were stored powered off until they were requested for patient use. With help from MM leadership, a plan was created to keep infusion pumps on while they were on the storage shelves waiting for delivery to patient care areas. Power strips were mounted to the storage shelves so the infusion pumps could be kept on and plugged in, which not only helped with drug library file uptake but also helped to keep batteries sufficiently charged for delivery to patient care areas. A key to this process was education of MM employees. MM staff were not familiar with pump operations and therefore needed instructions for how to turn the pumps on and get the pumps to the ready screen to allow for the drug library to be taken up while preventing the pumps from alarming as they sat on the shelves. Staff were also educated on powering off the pump prior to delivery to patient care areas so when the clinician powers on the pump, the new library can be activated by the normal workflow of selecting “new patient.”
Drug Library Name. The historical drug library name was structured with outdated abbreviations for the health system and the date in a “yyyy.mm.dd” format (e.g., UWHC 2016.02.05). This naming convention was not visually distinct or easily recognizable on the pump, which made it difficult for clinicians to determine the current library version. Using input from nursing councils and the Smart Pump Oversight Committee, the naming convention was simplified with the health system name and date written out for easier recognition (e.g., UW March 2023). It was important for the organizational name to be included in the drug library name as multiple health systems in the area use Alaris pumps and at times pumps are transferred with patients between locations. Differentiating UW Health pumps from outside hospital pumps is key to ensuring infusion safety, as formularies, drug library build, and interoperability functionality are unique to each organization’s pumps. Therefore, having UW in the drug library name added another quick way to distinguish UW Health pumps from outside hospital pumps. Furthermore, having the date spelled out versus in number format allows for quick recognition of the library name by frontline staff when evaluating library version during activation.
Pump Update Day. Prior to the evaluation of the drug library process, a drug library was released between the third and eighth days of the month. This was in alignment with the vendor’s suggestions for optimal infusion pump data retrieval; however, there was no standardization to the release date within that range and clinicians did not know when to expect the new library to be released. To optimize this, the drug library update day was assigned to the first Wednesday of the month that falls within the vendor’s recommended date range. This became known as “Alaris Pump Wednesday.” Wednesday was the preferred day of the week for managing the workload of the activation process, as the beginning and end of the week tend to be busier for nursing staff. The drug library release time was standardized to 9 a.m. to allow for communication at morning huddles to occur and for morning medication and rounding to complete. Finally, the drug library update dates are published on a nursing change impact calendar, which is a shared, organizationwide rolling calendar that contains important dates for patient safety initiatives.
Education. The drug library activation process is not automatic and requires effort by the end user to complete. Therefore, it is key to have proper education in place to ensure the process is followed.
For new employees, education is provided during nurse and nurse residency orientation. Nurses are taught how to use the infusion pumps, how to identify which drug library is on the infusion pump, and how to update the pump with the latest drug library version. Additionally, the aforementioned communication avenues are reviewed. Finally, the rationale and the importance of this process for patient safety are stressed.
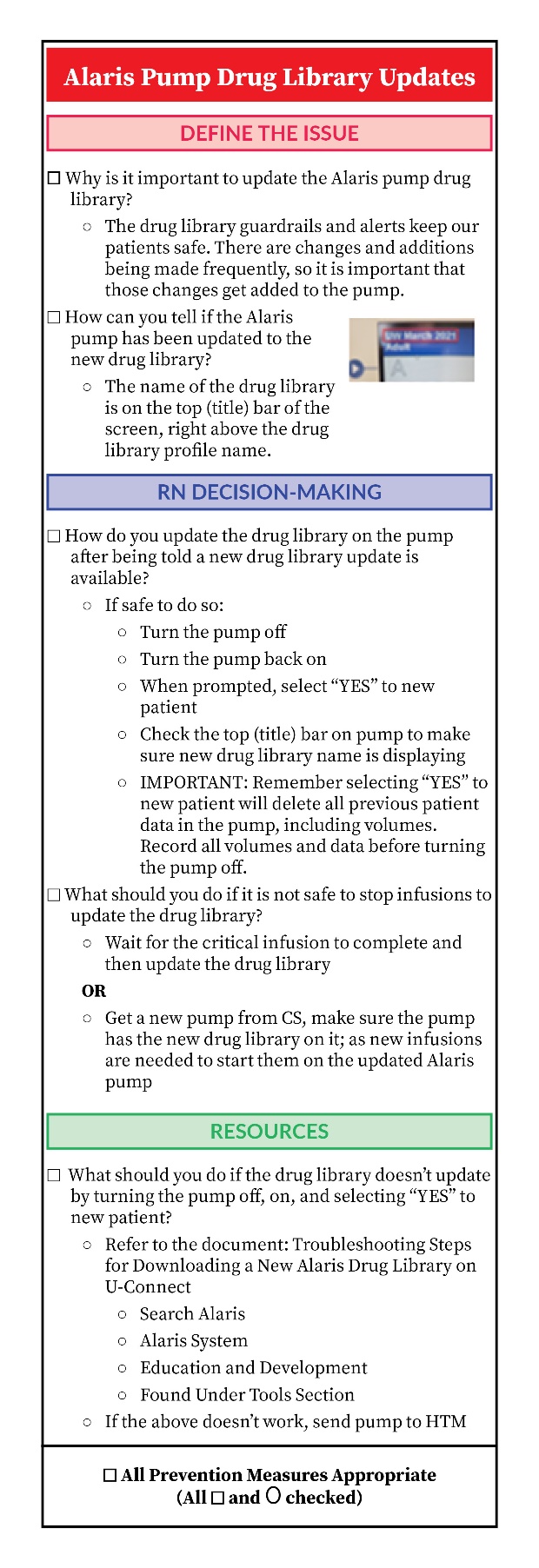
For current employees, continuing education on the pump update process was identified as a gap by nursing leadership and shared governance councils. To address this, a Kamishibai card (K-card) was created. K-cards are a recognized management tool that can be used to facilitate discussions between leaders and staff to improve processes.11 The UW Health Alaris pump drug library update K-card details the pump drug library activation process and the rationale for completing it, shows how to identify the current library version on the pump, and provides resources for troubleshooting problems (see Figure 2). It is included in the pump library update email sent out each month and is meant to be used by nursing leadership to reinforce the process.

Complex Patient Pump Update. After receiving feedback from clinicians that pump updates are difficult to complete on complex patients receiving continuous infusions that cannot be paused, a recommended workflow was designed for this subset of pumps that cannot be powered down easily to activate the library. Clinicians are instructed to either wait until the critical infusion has completed to update the pump, or request a new pump; ensure it is updated to the newest drug library; and as new infusion bags are hung, start them on the new updated pump.
Critical Library Updates. If a library update is required that will impact a medication concentration that is actively infusing on a patient (e.g., drug shortage changes), a process has been established with pharmacy and nursing to coordinate active order changeovers with the release of the updated drug library and direct communication to the affected end users. This coordination is done to ensure the new pump drug library file is activated and available to accommodate the new concentration to ensure patient safety.
Data Evaluation and Follow-Up. Another part of the improvement process was related to data evaluation. The BD Alaris platform uses a systems manager to track pump activation status. The systems manager produces a report that details the drug library transfer status. Prior to process improvement, the pump update progress was not routinely evaluated. During process optimization, a workflow for extracting this data at various time points after the library release was implemented to allow for tracking the activation status over time and comparing months to assess process improvement.
Initially, monitoring of the update status was based solely on the pumps that had the latest drug library activated, as compared to the pumps that were still working with an outdated drug library. However, after analyzing the information in this report more closely, it was determined we could drill down into the data even further to assess the drug library activation status on pumps that were powered on after the drug library release as compared to all pumps. By doing so, data points for pumps that are powered off or removed from the fleet were able to be filtered out, thus providing a more accurate picture of the drug library activation status of the pumps that are powered on and being used.
The next step in this data evaluation was sharing this data with clinicians as feedback to encourage and reinforce the workflow. As mentioned previously, this information is shared in organization huddles after drug library update day each month. Additionally, this information is provided to shared governance councils for awareness and the Smart Pump Oversight Committee for process improvement tracking.
Location of Outdated Pumps and Update of Pump Fleet Lists. When reviewing the data in the systems manager, it was noticed that some infusion pumps with outdated drug libraries had not connected to the server in a long time. These pumps were hypothesized to be either no longer in use or stored, powered off, in a remote location. To address this, a collaboration was formed with the UW Health biomedical engineering team, which has an asset management system, to locate those infusion pumps. If the pump was able to be located, the drug library was updated, and the pump was returned to circulation. If unable to be located, it was assumed the pump was no longer in use at UW Health and the pump was disregarded when reviewing the systems manager data. This allowed for more accurate pump activation data. This pump data evaluation and pump location analysis is completed periodically to maintain an accurate fleet list.
Scrolling Banner. As the improvement process progressed, feedback from clinicians suggested that additional communication to end users was needed to prompt activation of the drug library on the pump. In partnership with the UW Health Nursing Practice Council, it was suggested that a systemwide scrolling banner on UW Health computer workstations be displayed to remind clinicians to update the infusion pumps. On Alaris Pump Wednesday, a brief scrolling banner displays for clinical locations at two time points during the day to aid in this communication. The first banner runs from 10:30–11:30 a.m. and the second banner runs from 8–10 p.m. for clinicians on second and third shift.
Shared Governance Nursing Councils. Engagement of clinicians via shared governance councils was a key to many aspects of the quality improvement process. Involving clinicians in decision-making promotes collaboration, awareness of the issues, and accountability for follow-up. Additionally, this allows for recognition of issues that were not previously known and novel ideas for solving issues from those directly impacted.
Pharmacy/Nursing Partnership. Because the drug library update process involves both pharmacy and nursing, a key to success for all the strategies described is having a strong pharmacy and nursing relationship to manage the process. The expectation was established that a drug library update is needed to accommodate any changes to the formulary. Additionally, pharmacy and nursing collaborate on the management of all aspects of the infusion pump system, including building and testing of the drug library; follow-up on pump-related events, data analysis; and establishment of workflows related to infusion pump processes, such as the drug library update. Having a strong working relationship with effective communication facilitates the achievement of positive outcomes and aids in the day-to-day success of infusion pump management at UW Health.
Results
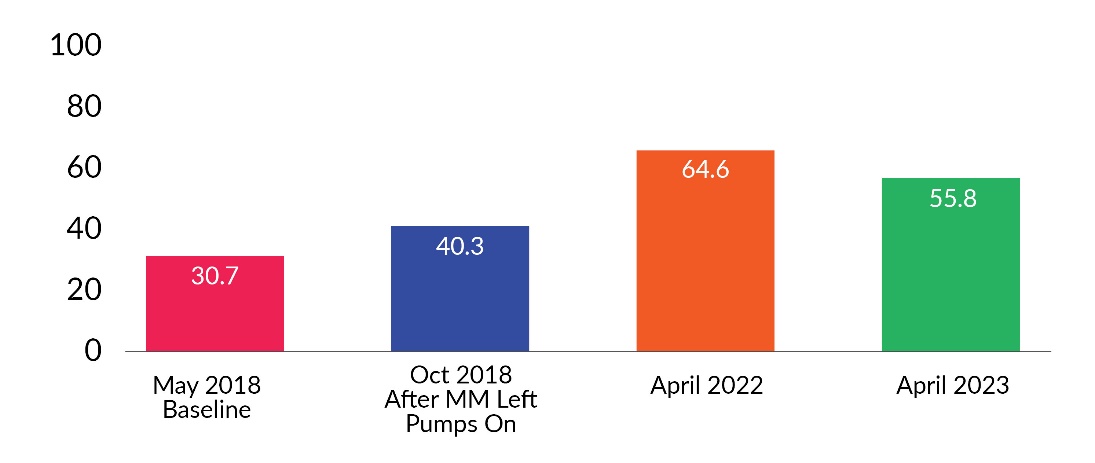
The percentage of pumps with the new library activated was tracked over time during the quality improvement process and key element implementation. See Figures 3, 4, 5, and 6 for activation percentages at days 1, 2, 5, and 9 after library release at various time points during the project. Pump update data prior to the next month’s library release was not consistently available; however, when end-of-month pump update data was available, the results demonstrated that over 90% of pumps were on the new library. Most recent data from December 2023 revealed 94.8% of our pumps were on the newest library before releasing the next one.




Discussion
In 2018, we evaluated our drug library activation data and ascertained there was no formal process in place for drug library updates or library activation. It was concluded there was a need to standardize the entire drug library update process, including workflows for activation of the drug library on the pumps, communication of the updates, and routine evaluation of data. The steps outlined in the article show the key process elements that our organization evaluated and the strategies implemented.
Establishing a strong interdisciplinary team with nursing informatics, pharmacy, biomedical engineering, and MM was a key initial step in this process. Specific collaboration between nursing and pharmacy was necessary to align formulary updates with the drug library updates. This required interdepartmental planning, coordination, and communication.
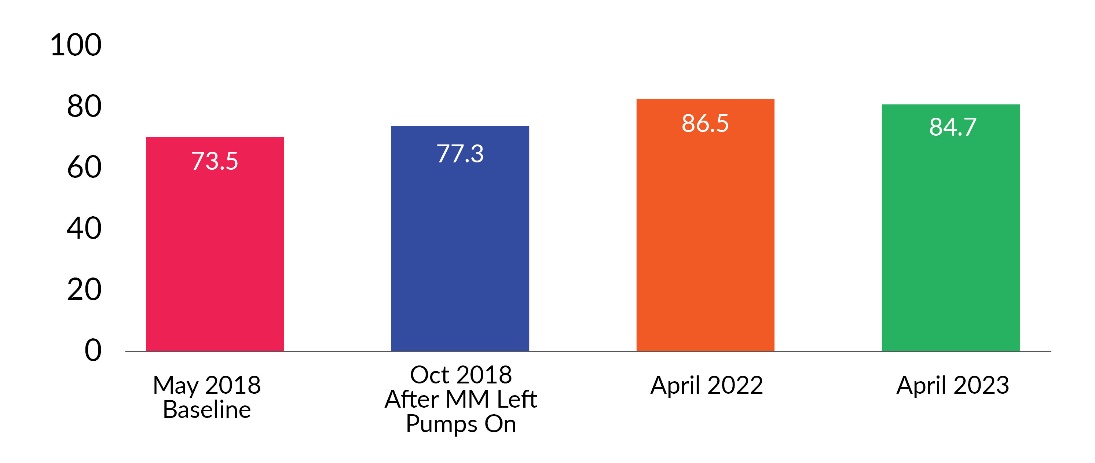
One of the earliest and most impactful interventions was working with MM colleagues to keep all pumps awaiting request by units powered on. This cross-functional teamwork identified a unique solution to improve the update process and resulted in more pumps being activated sooner than historically seen. With this intervention alone, we saw an approximate 10% increase in the number of pumps activated with the new library on days 1 and 2 after a library update was released (see Figure 7).

Another impactful strategy was education and engagement of end users on the importance of drug library updates. Involving nursing shared governance councils, Smart Pump Oversight Committee, and unit-based leadership to explore necessary steps helped improve understanding and buy-in. Effective communication utilizing multiple approaches allowed us to reach the broadest audience.
Data evaluation has been a continually evolving process. Initially the entire pump fleet was evaluated for drug library update activation; however, after critically analyzing the available data, it was determined that separating out powered-on and active pumps provided a better sense of the activation status of pumps being used on patients. This became the focus of the efforts to improve patient safety. We now track two sets of data, one set for the entire pump fleet and another for the active pumps to get a broader sense of overall drug library activation status.
Data presentation and report-outs to nursing leadership and end users continue to reinforce the need for and importance of the process and highlights the efforts by nursing staff to update the drug library on the pumps.
Limitations
For Alaris pumps, the process for drug library activation is manual and requires a conscious effort by end users to complete. This workflow is burdensome on end users given the myriad of and continual addition of competing responsibilities placed on them during patient care. Overcoming this additional workload and sustaining the change effect is challenging and has potentially led to waning activation rates over time (see Figures 3, 4, 5, and 6). A more automatic, end-user-independent pump library activation process is needed to address this issue.
In addition to the workload associated with monthly updates, unscheduled library updates to accommodate drug shortages or urgent library changes add to the end-user burden. This has affected UW Health over the recent past, and due to recent supply chain issues and the growing number of medication shortages, it will likely continue to impact organizations and infusion safety. Therefore, it is important for organizations to develop a process to address this and ensure timely drug library activation to accommodate these critical changes.
Another challenge our organization faces with the process is that powered-off pumps cannot take up the latest drug library. Locating these pumps to update them is difficult and time-intensive and can lead to lower pump update numbers and outdated drug libraries. Having the ability for uptake of the library file when the pump is powered off would help.
Finally, evaluation of pump activation is laborious, especially when trying to separate pumps that may no longer be in circulation. Another obstacle with data evaluation is the inability to pull historical data. Data can only be pulled for the present time. As the focus of our data analysis has changed over time, this has led to some inconsistency in reportable data.
Conclusions
It is essential that organizations establish a process to update their smart infusion pump libraries. With current pump limitations, it is necessary to have a framework in place to ensure timely activation of the new drug library for patient and medication safety. Establishing a strong interdisciplinary team to create and implement a standard workflow is key, along with broad communication and follow up to engage end users. It is also critical to track and evaluate data and continually assess other strategies that may improve the process.
Ideally, infusion pumps would allow for seamless drug library updates with little to no impact for the end users. This should be the goal for the infusion pump market. However, in the interim, organizations need to focus on optimizing their drug library update process to ensure patient safety.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
Courtney Olson (colson@uwhealth.org) is a nurse informaticist who manages smart pump workflows and infusion practices at UW Health.
Carin Bouchard is a clinical pharmacist who manages the smart pump drug library at UW Health.