Introduction
Wrong-site surgery (WSS) remains a significant and avoidable medical error, persisting despite decades of national and international efforts to prevent it. While the development and implementation of safety protocols—such as the Universal Protocol1 and World Health Organization Surgical Safety Checklist2—likely have helped to prevent WSS events, these “never events” still occur across a range of settings, including hospitals and ambulatory surgical facilities.3–15
Pennsylvania is one of the few large governments or entities that mandates reporting of patient safety events ranging from near misses to serious events.3 Therefore, all licensed healthcare facilities, including acute care hospitals and ambulatory surgical facilities (ASFs) in Pennsylvania are required by law16 to report WSS events to the Pennsylvania Patient Safety Reporting System (PA-PSRS)[1] database. The combination of mandated reporting and a long-standing database have allowed the Patient Safety Authority (PSA) to develop a notable history of exploring, studying, and publishing on WSS,3,17–31 and we continue that practice by providing an updated and in-depth analysis of WSS event reports.
In this study, we utilized the PA-PSRS database and expanded upon our prior WSS research3 by examining events over a recent 10-year period. This expanded time frame allows for the analysis of a substantially larger sample of WSS events across the following clinically related variables: facility type, hospital procedure location, hospital bed size, clinician specialty, body region, specific body part, procedure group, and specific procedure. The present study will include novel cross-tabulations with the purpose of providing a deeper understanding of how WSS varies across different contexts. The findings are intended to inform stakeholders and support the development of targeted strategies to prevent WSS events.
Methods
Data Source and Sample
Data were obtained from patient safety event reports submitted by hospitals and ASFs to the PA-PSRS acute care database, which operates under Pennsylvania’s mandatory event reporting laws. These reports contain both structured fields (e.g., event date, patient age, and care area) and unstructured fields (i.e., free-text entries), which allow reporters to describe the event and any actions taken. The de-identified reports do not contain medical records.
The identification and review of events for inclusion in this study were conducted in two distinct phases. During the first phase, the PA-PSRS database was queried for events that occurred over a 10-year period (January 1, 2015, to December 31, 2024) and satisfied one or more of the following inclusion criteria:
-
Event was classified within the PA-PSRS taxonomy as an Error Related to Procedure/Treatment/Test - Surgery/Invasive Procedure Problem and one of the following event subtypes was selected: wrong site, wrong side (L vs R), wrong procedure, wrong patient, or preparation inadequate/wrong.
-
Event was classified within the PA-PSRS taxonomy as Error Related to Procedure/Treatment/Test - Surgery/Invasive Procedure Problem and at least one of the unstructured fields contained the words “left” and “right” or “incis” and “excis”[2].
-
Event was classified under the Surgical Services care area group[3], and at least one of the unstructured fields included variations of one or more of the following phrases: wrong site, wrong side, wrong level, wrong procedure, wrong patient, time out, incorrect side, incorrect site, incorrect procedure, incorrect patient, block, or mark.
In the second phase, a researcher conducted a review of each report to determine whether it met the inclusion criteria by describing an invasive operative procedure and a WSS. (See Table 1 for definitions along with examples of WSS organized by error type.) A total of 664 event reports were selected for inclusion in the study and 367[4] of those event reports were included in our previous article about WSS during 2015–2019.3
Design, Analysis, and Variables Coded
We conducted a retrospective mixed-methods study using an exploratory sequential approach,32 beginning with an analysis of qualitative data, which were subsequently quantified for further examination. The qualitative data from PA-PSRS event reports were examined using directed content analysis,33,34 applying the framework method32,35,36 with variable categories guided by our previous research.3,17 The variables were quantified by frequency and evaluated through descriptive analysis. Descriptive analysis is a quantitative approach used to explore phenomena and identify patterns, aiming to improve understanding and explanation of their occurrence.3,37 This is often achieved through visual analysis of displays of data that illustrate multiple variable combinations and enable the triangulation of insights.
For each event report, the patient’s age, patient’s gender, event date, facility type, and facility bed size were extracted from the structured fields. From the unstructured fields in the event reports, a researcher manually reviewed and coded the following variables: hospital procedure location (three categories), error type (four categories), clinician specialty (23 categories; the spinal surgery category consists of orthopedic surgeons and neurosurgeons who performed spinal procedures), body region (12 categories), body part (41 categories), procedure group (11 categories), and specific procedure (34 categories). Consistent with our previous study of WSS,3 the variables were coded for what occurred during the event, not what was intended. For example, the researcher coded each event based on the procedure performed and the body region affected, which could have differed from the intended procedure or body region. For a description of the hierarchy in selection of codes per variable, see the methods section in our previous study.3 All coding assigned to events from 2015–2019 remained unchanged from our previous study, unless an opportunity to improve accuracy and reliability of codes was identified.
Results
In addition to the figures and tables presented throughout the body of this manuscript, we also provide results in Online Supplement Appendices S1–S9. These appendices present WSS findings through various cross-tabulations of the following variables: year of event occurrence, facility type, error type, clinician specialty, body region, specific body part, procedure group, and specific procedure. Presenting the findings through multiple visualizations and variable combinations is intended to offer stakeholders a more comprehensive understanding of the patterns and characteristics of WSS events.
Patient Gender and Age
Patient gender was identified in 95% (633 of 664) of the reports and among those, 55% (347 of 633) were female and 45% were male (286 of 633). Across the sample, patient age was a mean of 57 years and a median of 60 years (minimum was 0 years, 25th percentile was 48 years, 75th percentile was 72 years, and maximum was 99 years).
Wrong-Site Surgery by Facility Type, Hospital Procedure Location, and Hospital Bed Size
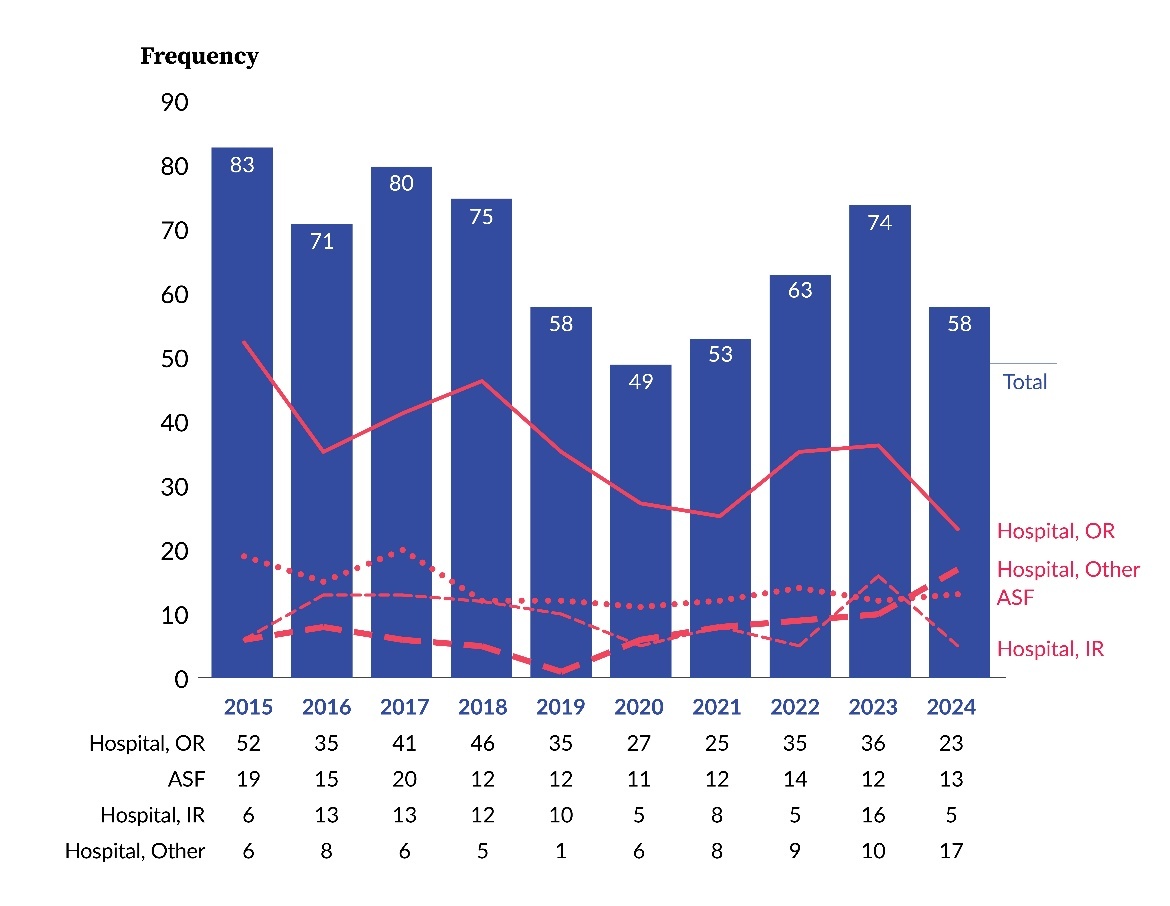
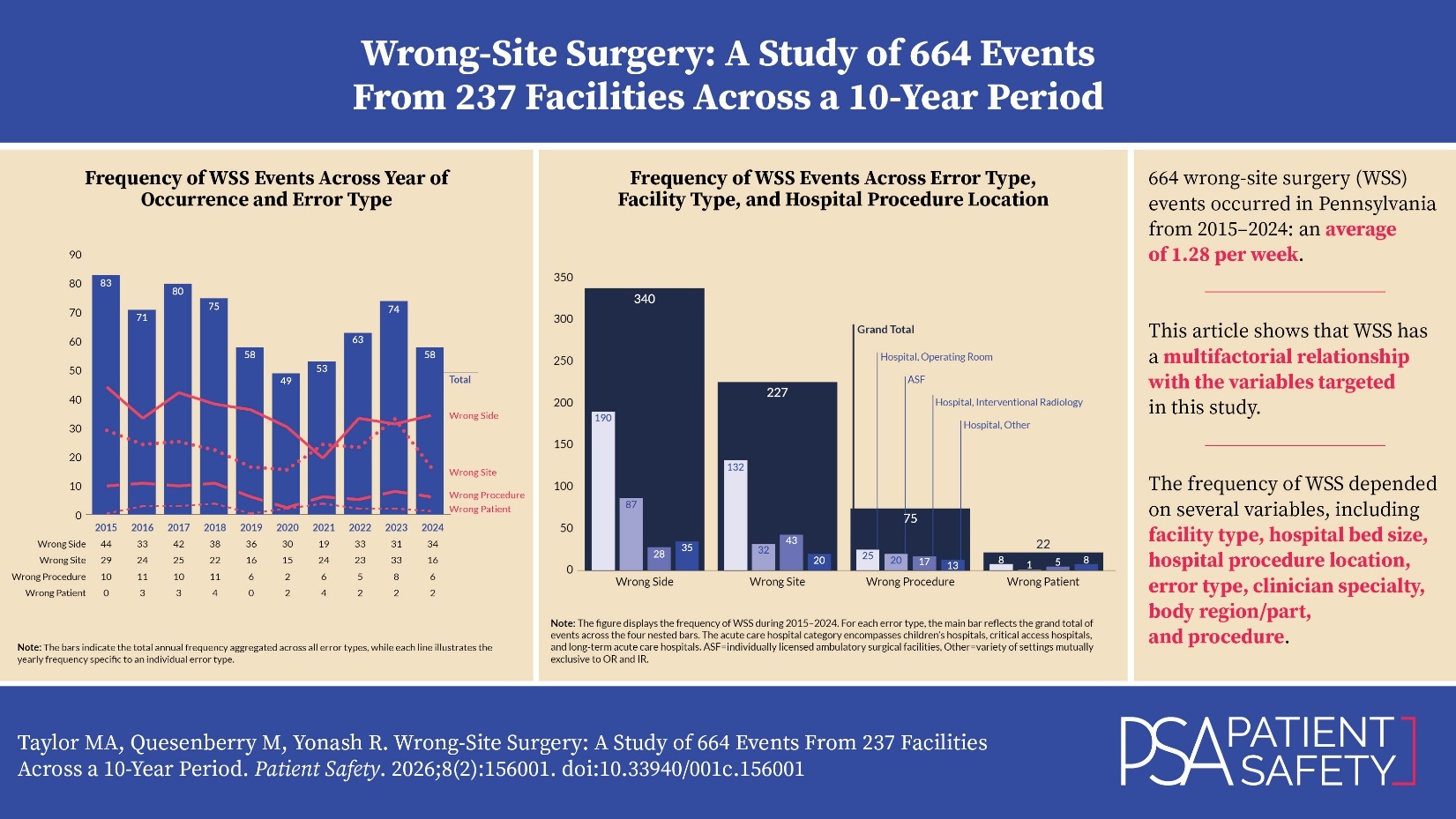
Figure 1 shows the occurrence of WSS events, across a 10-year period, at both individually licensed acute care hospitals and ASFs[5]. The total annual frequency of WSS varied over time, peaking at 83 events in 2015 and reaching a low of 49 events in 2020. The majority of WSS events were associated with hospitals rather than ASFs and were distributed across operating rooms (ORs)[6], interventional radiology (IR), and other[7] procedural locations. Within hospitals, the frequency of WSS was consistently higher in the OR compared to IR; however, IR reported between five and 16 WSS events annually throughout the study period. ASFs reported WSS events every year, with a maximum of 20 events in 2017 and a minimum of 11 events in 2020.
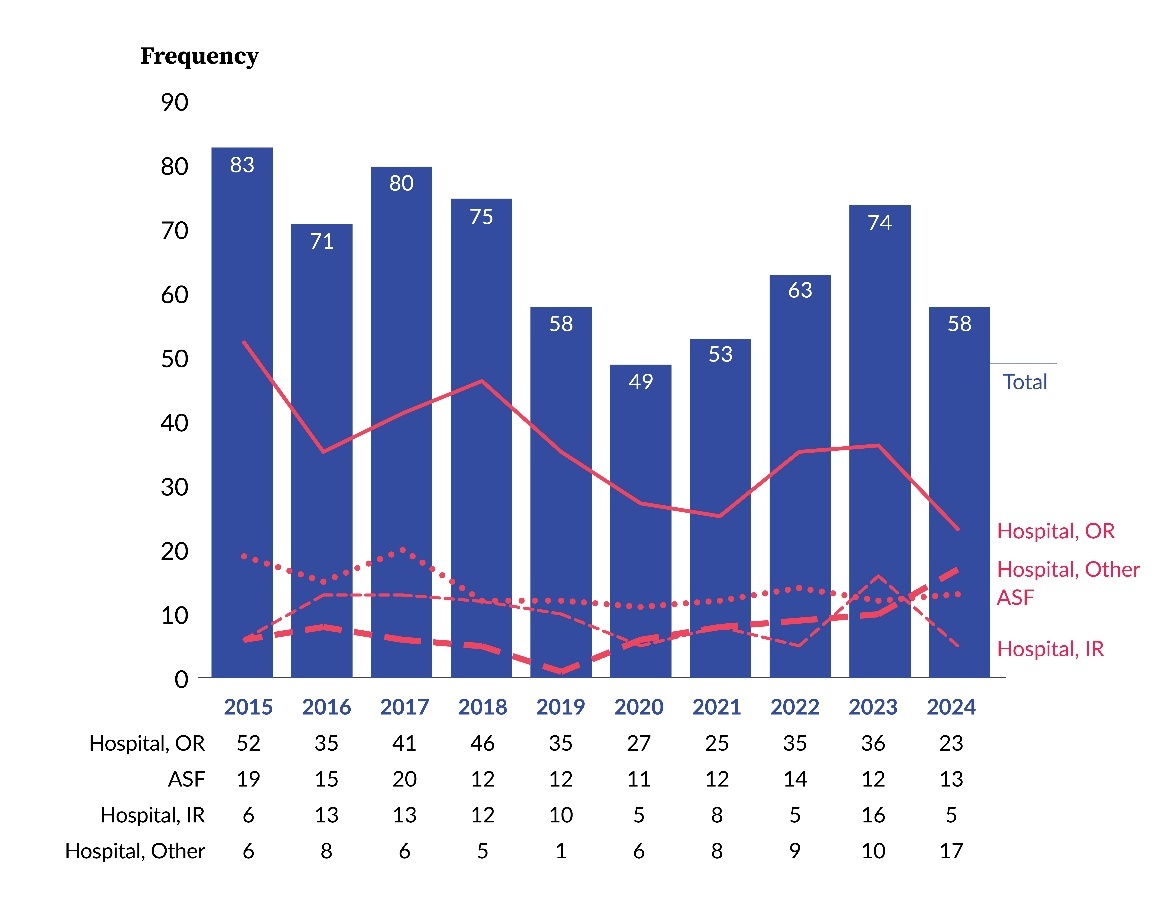
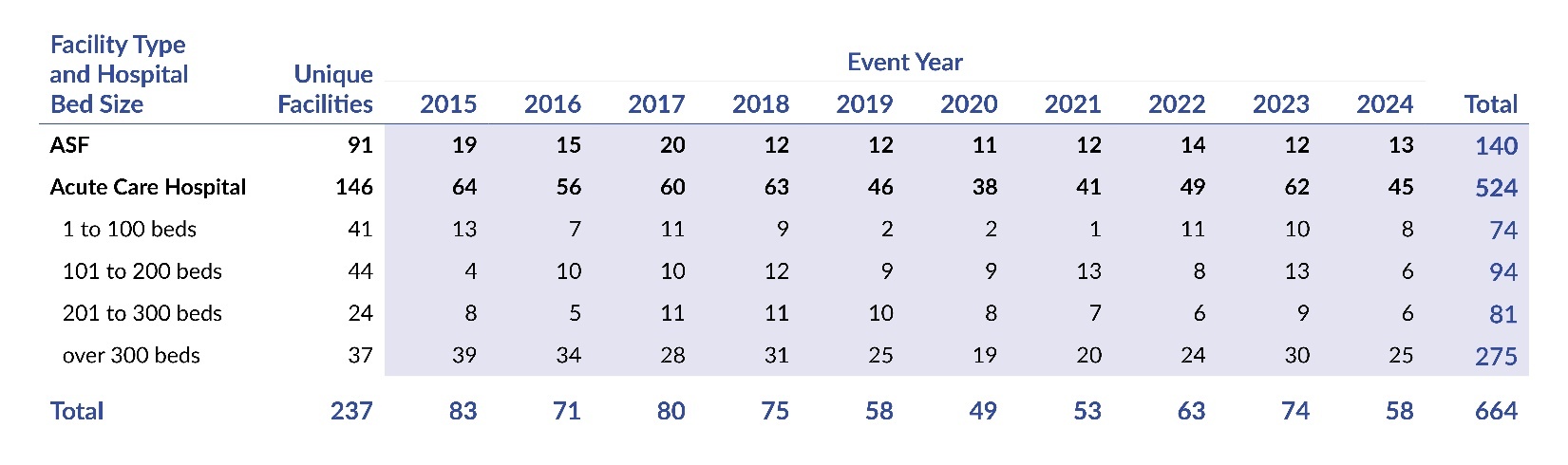
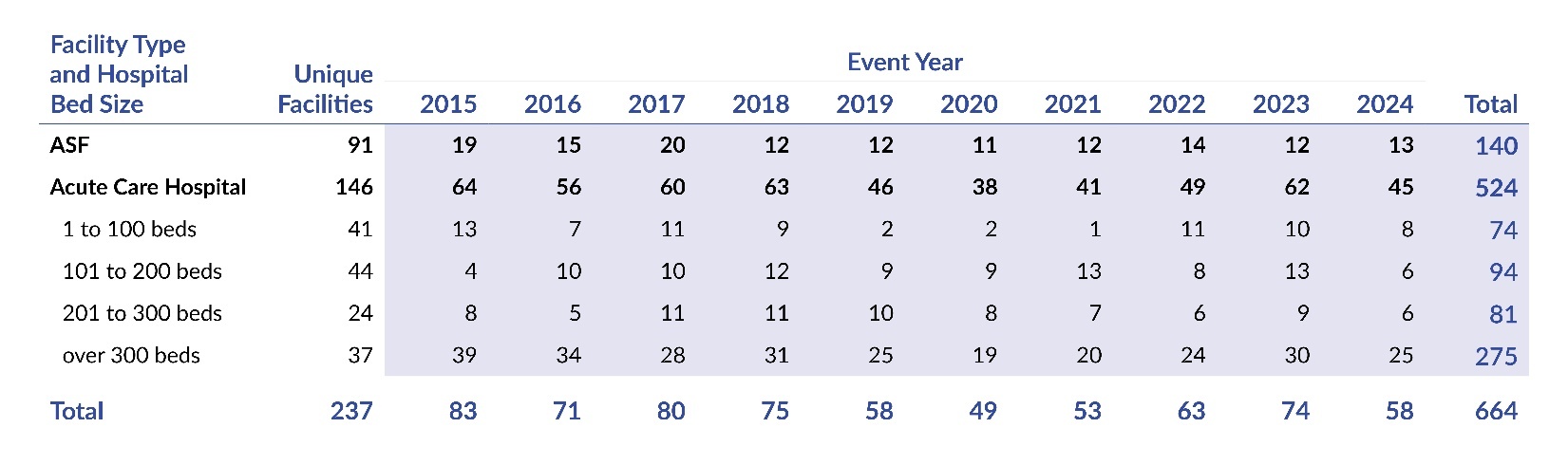
Table 2 presents the distribution of WSS events by year, facility type, and hospital bed size. Hospitals were the setting for the majority of WSS events, accounting for 79% (524 of 664), and hospitals having more than 300 beds were 41% (275 of 664) of the total. In comparison, ASFs reported 21% (140 of 664) of WSS events.
Table 2 also reveals the number of unique facilities that reported at least one WSS event during the 10-year period. During 2015–2024, 91 ASFs had at least one WSS, a range of 1 to 5 (mean=1.5; median=1), with 34 ASFs reporting two or more. We also found that the 146 acute care hospitals reported a range of 1 to 28 WSS events, a mean of 3.6, and a median of 2 (64 hospitals reported three or more WSS events).
Wrong-Site Surgery by Error Type and Other Clinically Related Variables
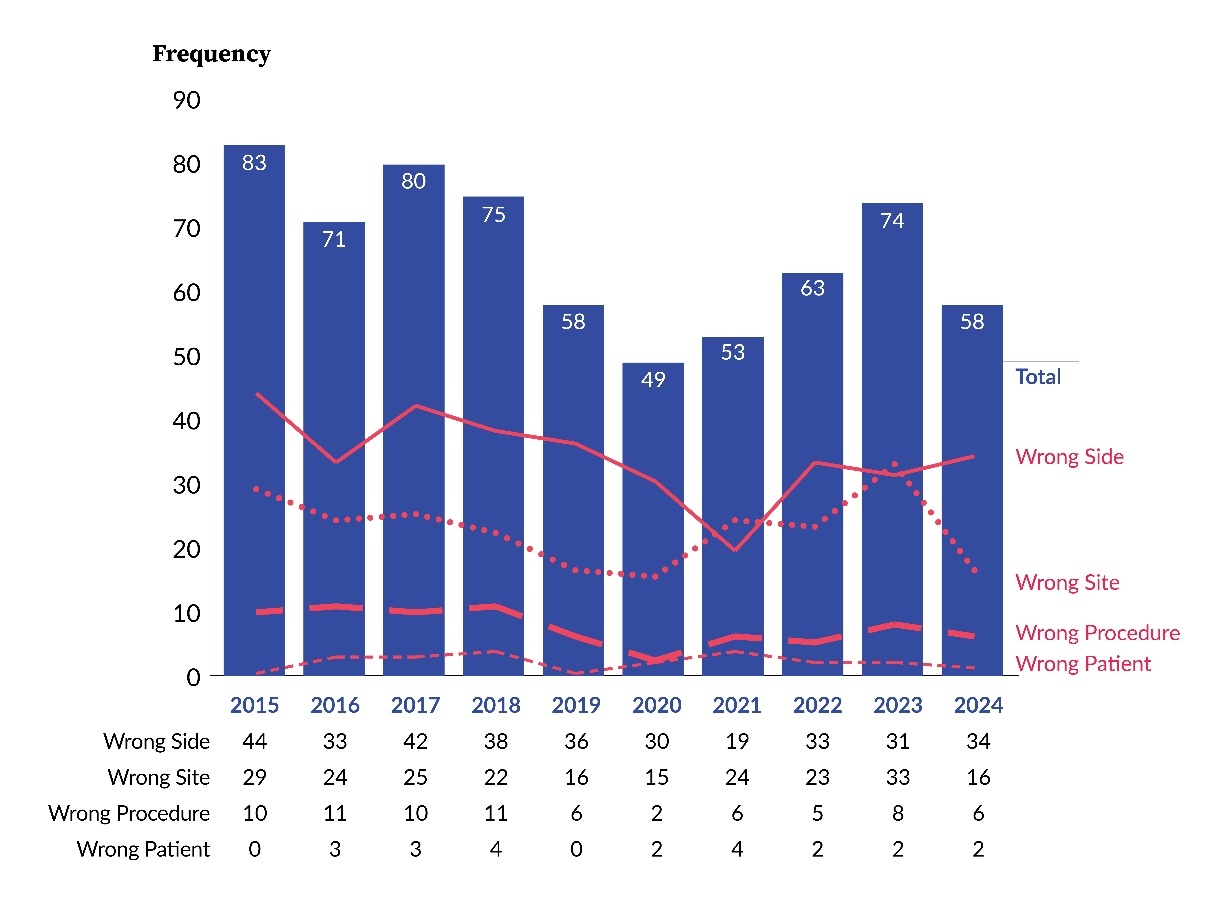
Figure 2 shows that wrong-side errors were the most common error type during eight of the 10 years, while wrong-site errors were the most frequent in the remaining two years. Across the 10-year period, the error types had the following distribution: 51% (340 of 664) were wrong side, 34% (227 of 664) were wrong site, 11% (75 of 664) were wrong procedure, and 3% (22 of 664) were wrong patient. The figure reveals, based on visual analysis of the data, that the frequency of each of the error types was variable and without a clear trend.
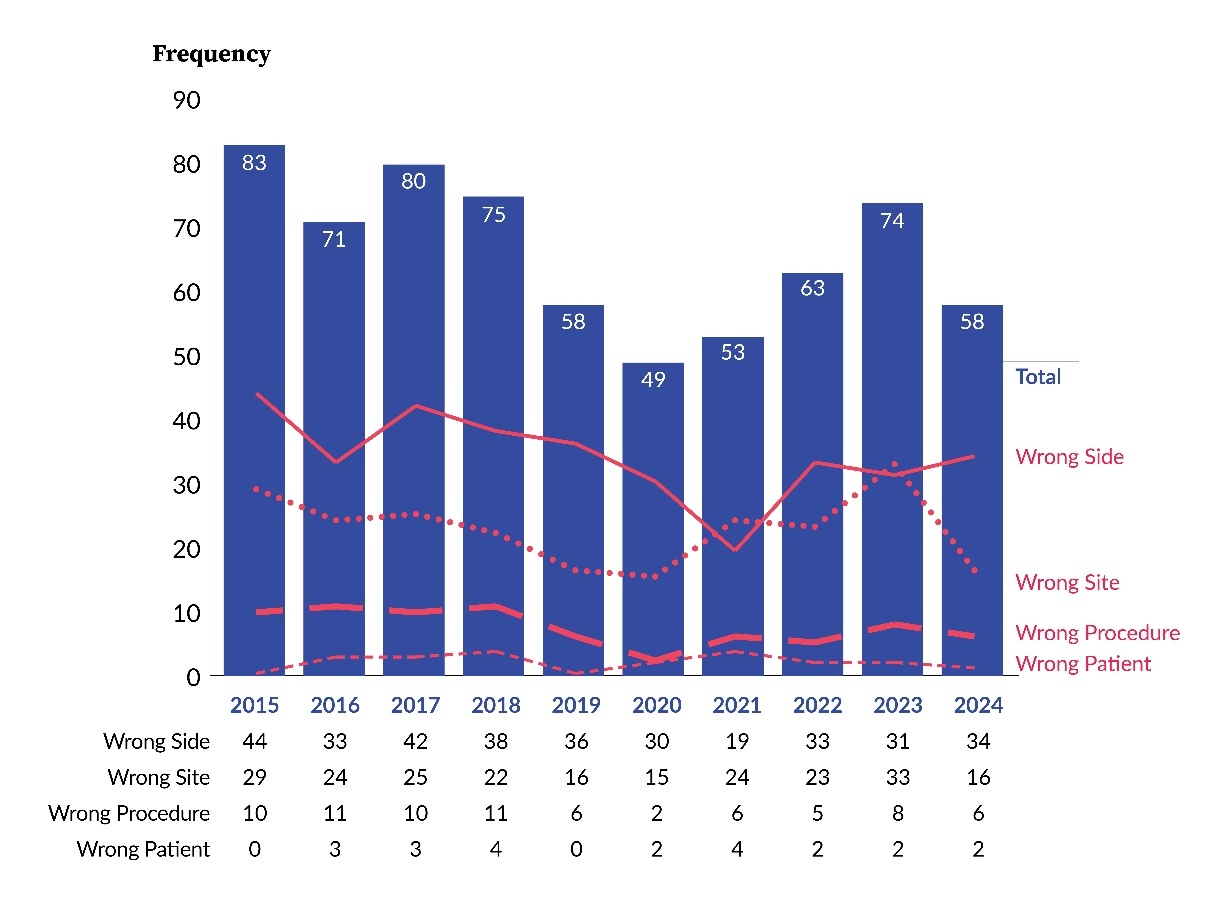
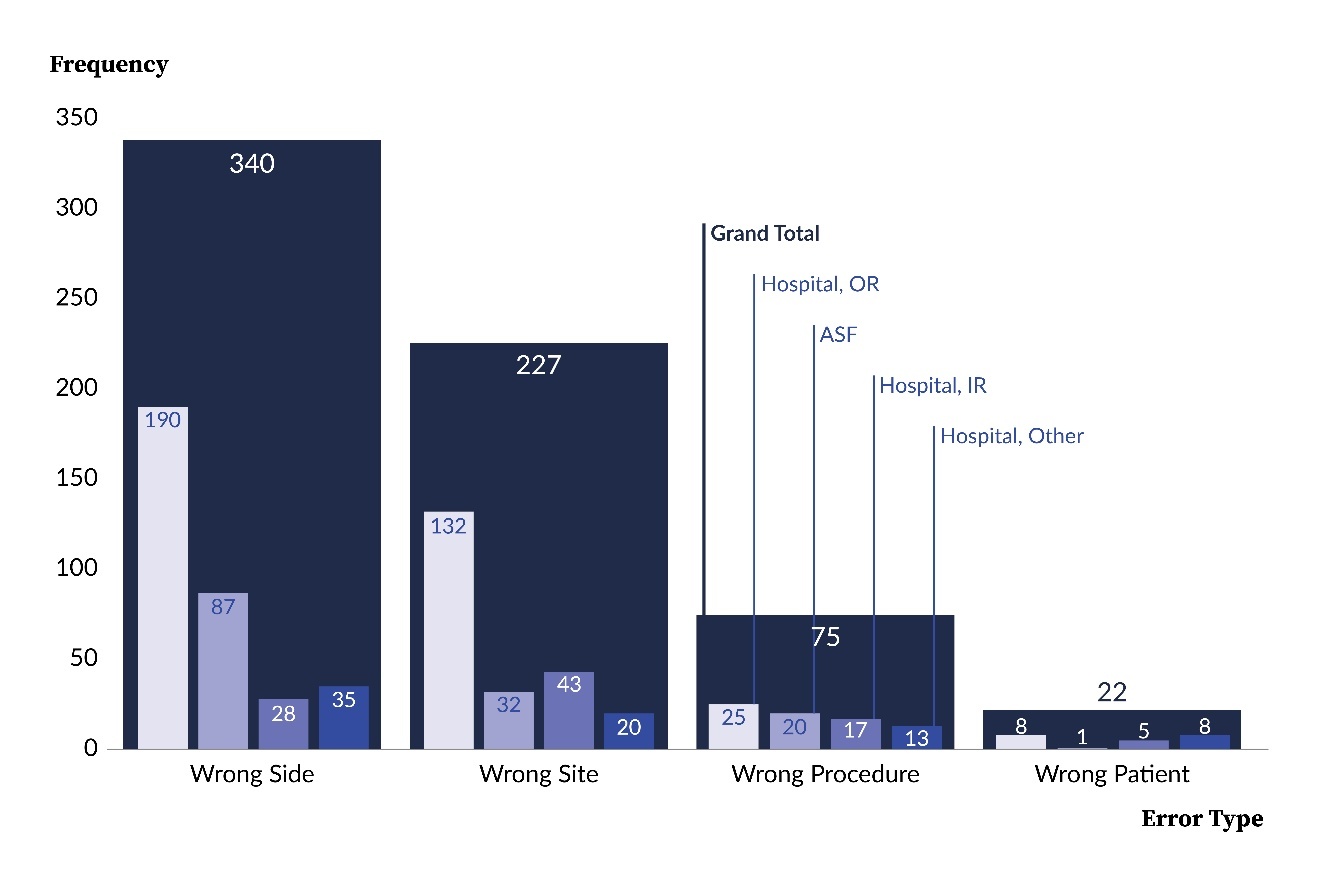
Figure 3 illustrates observable differences in the distribution of WSS error type dependent on facility type and hospital procedure location. For instance, wrong-side errors accounted for 62% (87 of 140) of WSS events at ASFs and 48% (253 of 524) at hospitals. In contrast, wrong-patient errors comprised 4% (21 of 524) of hospital events and less than 1% (1 of 140) at ASFs. As another example, within the hospital facility type, ORs reported 68% (132 of 195) of the wrong-site errors, but only 45% (25 of 55) of the wrong-procedure errors. Collectively, these findings suggest that the likelihood of specific error types may vary depending on both the facility type and the procedural location within hospitals.
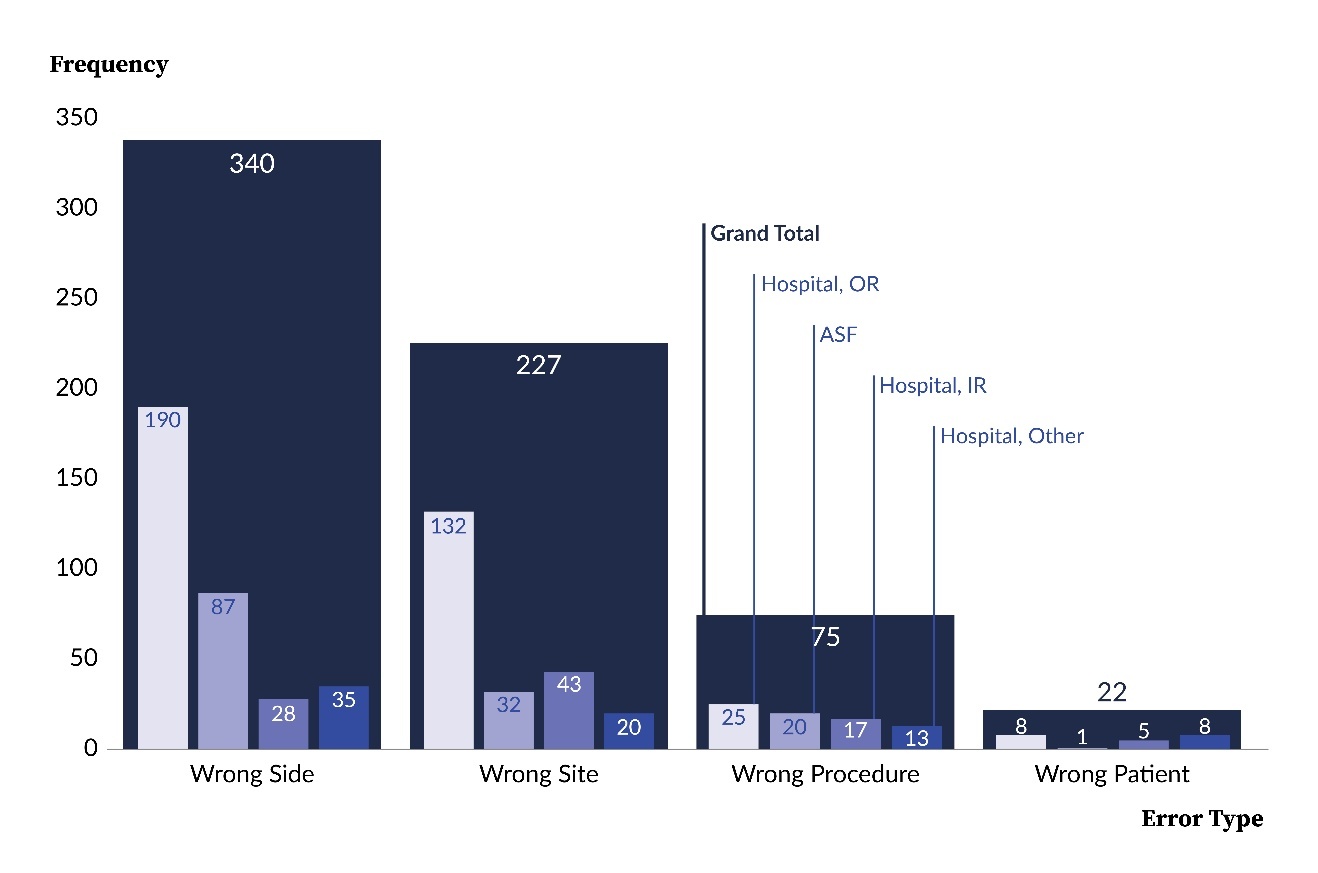
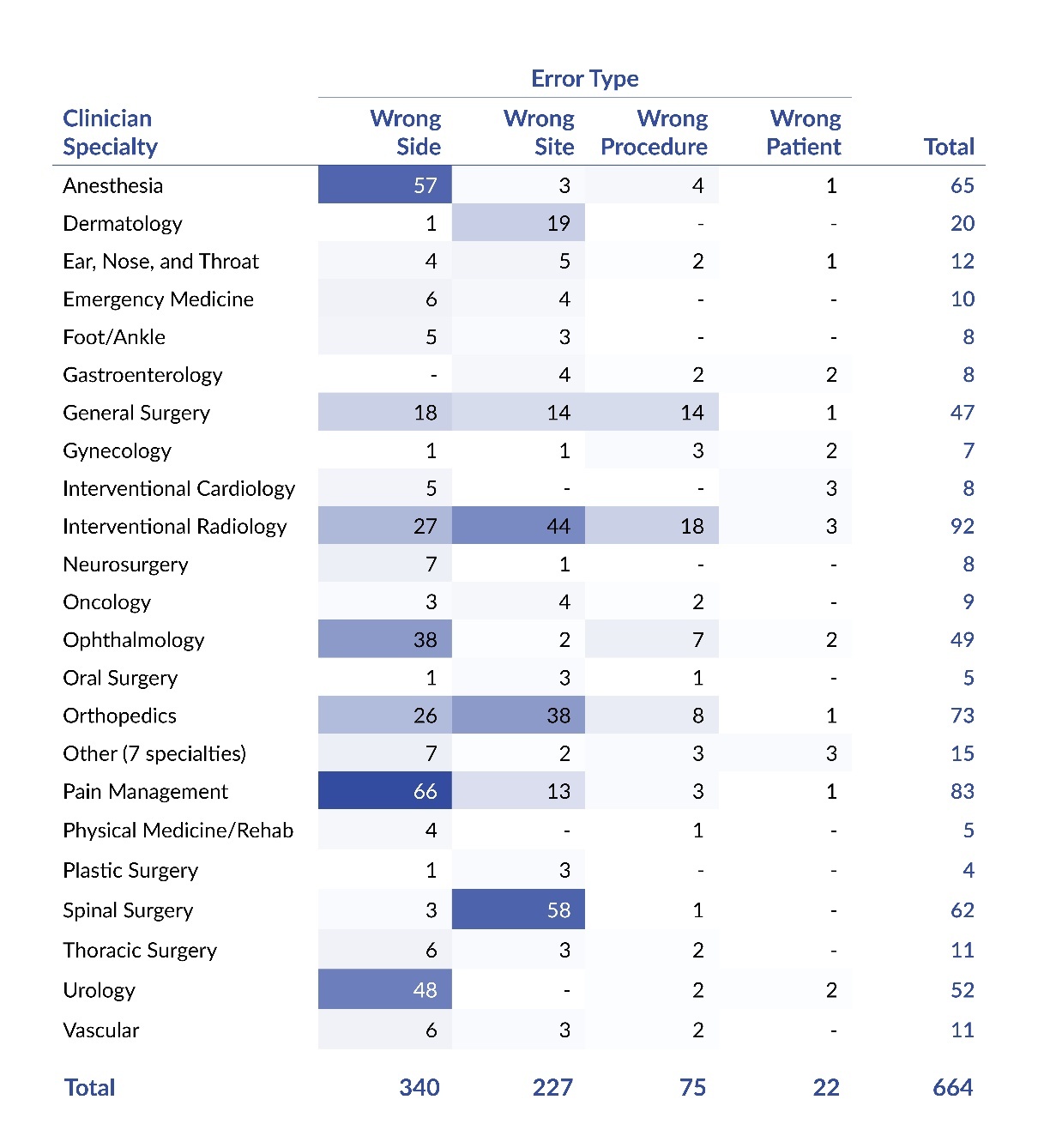
Table 3 displays the distribution of WSS events by error type and clinician specialty. The most frequently involved specialties were interventional radiology (14%, 92 of 664), pain management (13%, 83 of 664), and orthopedics (11%, 73 of 664). The table shows that certain specialties were associated with a broader range of errors, while others were largely related to a single error type. For instance, spinal surgery was overwhelmingly associated with wrong-site errors, accounting for 94% (58 of 62) of events reported by that specialty. In contrast, interventional radiology reported a relatively high percentage of multiple error types, including wrong-site (48%, 44 of 92), wrong-side (29%, 27 of 92), and wrong-procedure errors (20%, 18 of 92).
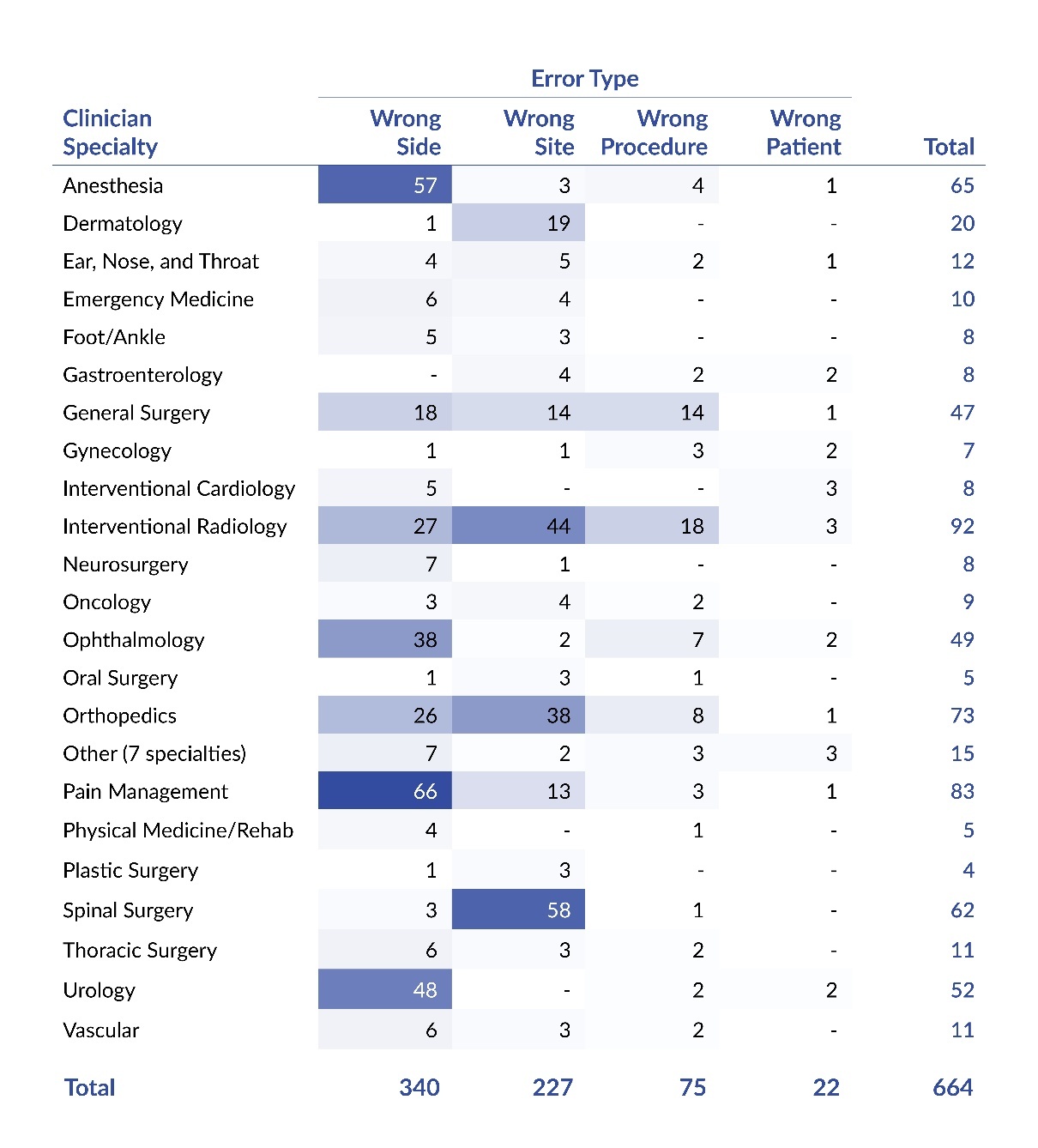
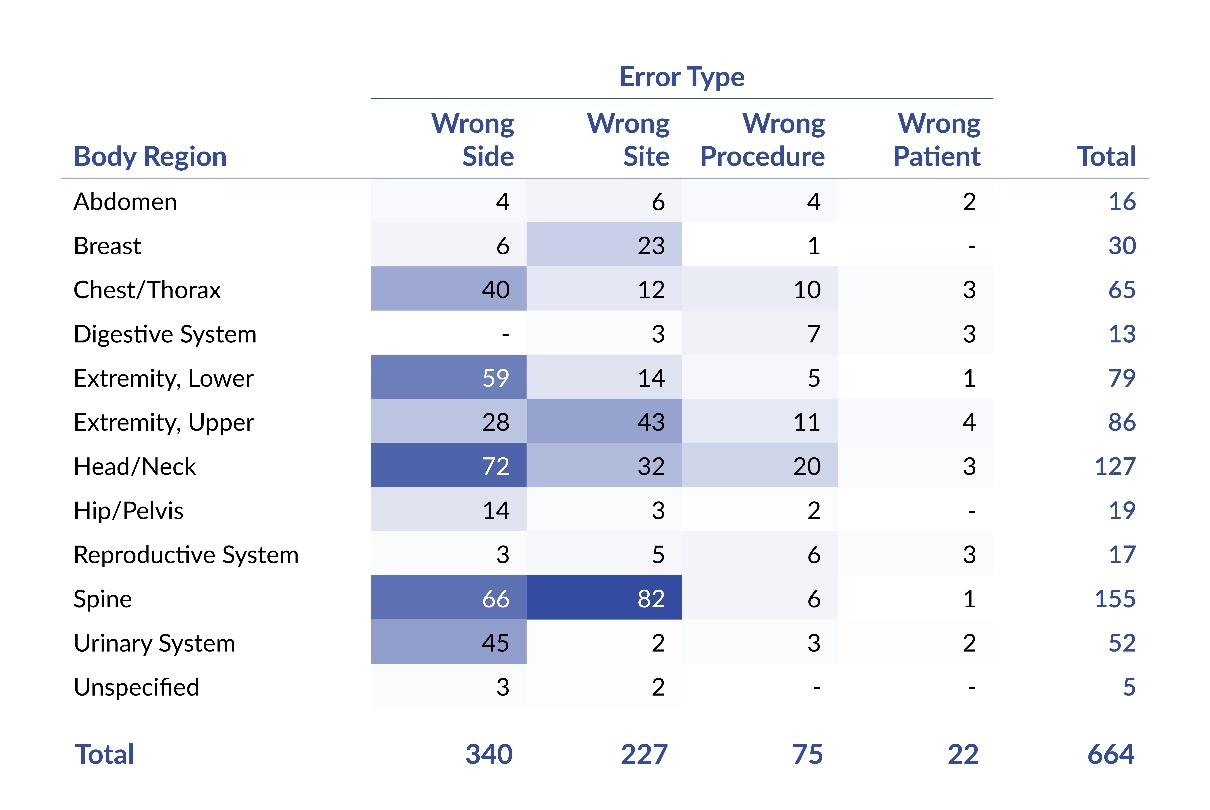
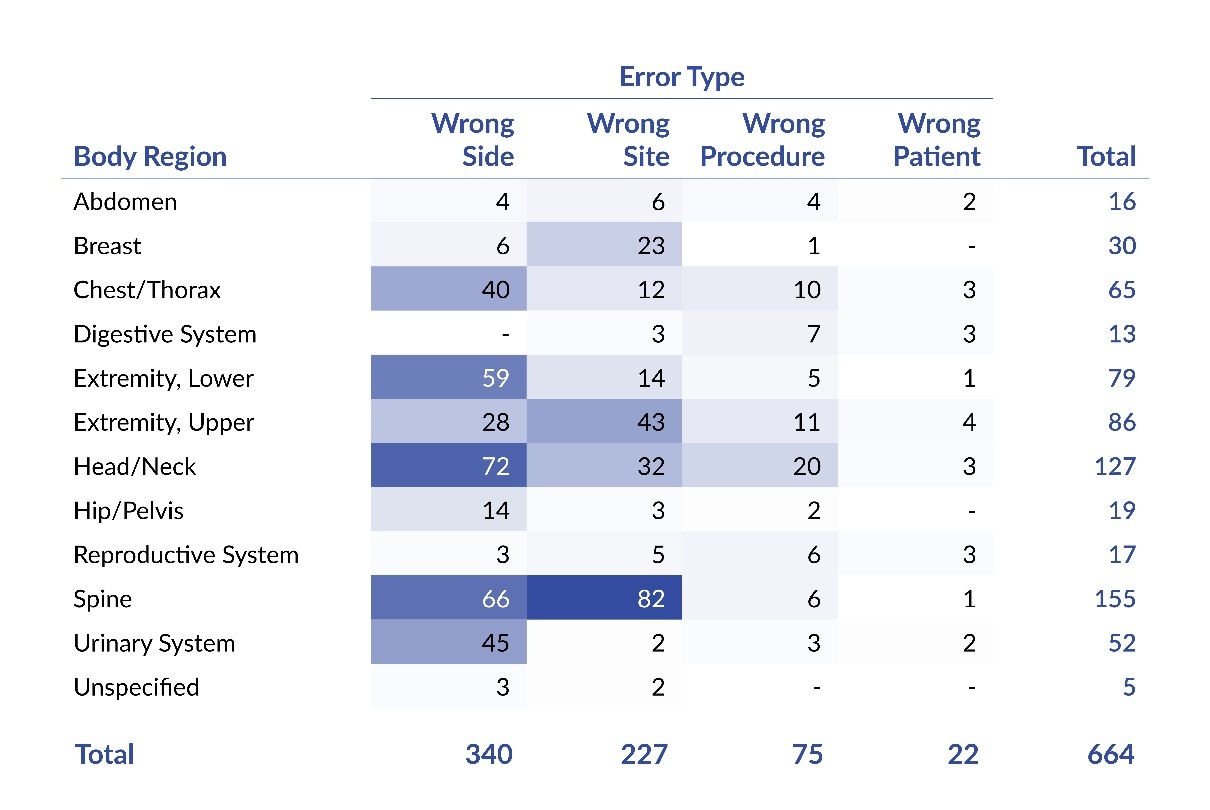
Table 4 reveals that the most commonly affected body regions were the spine (23%, 155 of 664), head/neck (19%, 127 of 664), upper extremity (13%, 86 of 664), and lower extremity (12%, 79 of 664). The data also suggests that some body regions were associated with a variety of error types, whereas others tended to be related to a single type. For instance, WSS events involving the head and neck region frequently consisted of wrong-side (57%, 72 of 127), wrong-site (25%, 32 of 127), and wrong-procedure errors (16%, 20 of 127). In contrast, the urinary system was primarily associated with wrong-side errors (87%, 45 of 52).
To gain a deeper understanding of the characteristics of WSS events, we analyzed the frequency of WSS by specific body part within each body region, as detailed in Online Supplement Appendix S5. Of the 664 event reports reviewed, 34 did not specify the affected body part. Among the remaining 630 reports, 62 distinct body parts were identified as being involved in WSS events. Within each anatomical region, one specific body part accounted for approximately one-third or more of the reported events. For instance, in the chest/thorax region, the pleural cavity was involved in 49% (32 of 65) of the events. Similarly, in the lower extremity region, the knee was associated with 42% (33 of 79) of the events. These findings suggest that certain body parts may be more susceptible to WSS events than others.
Table 5 reveals the relationship between error types, procedure groups, and specific procedures. The procedure groups most frequently related to WSS events were injections (31%, 204 of 664), spinal (12%, 82 of 664), and vascular (8%, 56 of 664). The data suggest that while some procedure groups were associated with a wide range of error types, others were predominantly associated with a single category. For instance, vascular procedures were linked to all four error types, whereas urological procedures were almost exclusively associated with wrong-side errors. Additionally, the table highlights patterns in the types of errors linked to certain procedure groups—for example, lower extremity orthopedic/podiatric procedures were for the most part associated with wrong-side errors, while upper extremity orthopedic procedures were primarily linked to wrong-site errors. Finally, wrong-procedure and wrong-patient errors were the least common overall. Notably, vascular procedures accounted for the largest share of both wrong-procedure errors (29%, 22 of 75) and wrong-patient errors (27%, 6 of 22).
In Table 5, we further analyze the distribution of WSS events within each procedure group by compiling the frequency of specific procedures. Within the total sample of WSS reports, 13 lacked sufficient detail to determine the specific procedure performed and were categorized as unspecified. Among the remaining reports (651 of 664), 117 unique procedures were identified as being associated with WSS events. Blocks (anesthetic/pain) emerged as the most frequently reported specific procedures across all events. In nearly every procedure group—except for lower extremity orthopedic/podiatry and the “other” category—one specific procedure accounted for at least 35% of the WSS events within that group. For example, spinal decompression/stabilization (e.g., discectomy, laminectomy, foraminotomy, corpectomy, and fusion) alone were linked to 60% (49 of 82) of WSS events involving spinal procedures.
It is important to note that the number of WSS events reported for each procedure group in Table 5 may be lower than the corresponding frequency in the body region categories presented in Table 4. These discrepancies are due to the procedure groups being categorized independently of clinician specialty or anatomical location. For instance, Table 4 reports that 155 WSS events involved the spine region, while Table 5 reports 82 events within the spinal procedure group. This difference is attributable to nearly half of WSS events that occurred in the spine region but were classified under other procedure groups, such as biopsy, excision, or injection. For a cross-tabulation of WSS events by procedure group and body region, refer to Online Supplement Appendix S9.
Discussion
As demonstrated by the current study and numerous recent studies of WSS,4–15 these “never events” persist as a substantial challenge within the healthcare community despite decades of effort to improve education, awareness, and perioperative intervention. The present WSS study expands upon our previous study3 by extending the observation period from five to 10 years and including visuals that allow for analysis of novel combinations of variables. The present study also helps to characterize the occurrence of WSS in a more comprehensive manner by using a large sample of facilities. To our knowledge, this study, with a sample of 664 WSS events across 237 hospitals and ASFs, is the second largest sample of WSS events examined in a single study, following a prior PSA study.30
Since our last study and review of WSS literature,3 we identified 12 additional studies published in recent years.4–15 These studies varied most notably by data source, time period of events, number of institutions reporting events, types of clinician specialties/procedures included, severity of outcome, and coding of clinically related variables. Due to the methodological differences, none of the 12 studies allow for a full comparison with our findings. For example, to the best that we can determine, only our study systematically explored the relation between WSS and facility type, hospital procedure location, and hospital bed size.
In the current study, there was a high degree of fluctuation in the frequency of WSS events across the 10-year period, and the lowest frequencies corresponded with a period of heightened challenges and concern associated with COVID-19 (i.e., coronavirus disease 2019).43,44 The decrease in the average number of WSS events per week from 2015–2019 (1.41 WSS events per week) to 2020–2024 (1.14 WSS events per week) likely is at least in part explained by a reduction in procedures being performed during 2020 and 2021.45 The decline in WSS reports during 2020 and 2021 resembles a pattern reported by other studies of WSS events.8,12 Overall, based on visual analysis of the data, there was no discernable trend, increasing or decreasing, in the frequency of WSS events across the 10-year period.
Per subcategory of variable targeted in the current study, it is difficult to conclude whether or not there is a true change in trend due to the relatively low volume of event reports. For example, wrong-procedure errors were a frequency of 10 to 11 per year during 2015–2018 and five to eight per year in 2021–2024. While this finding may suggest that there is a downward trend across the 10-year period, the small number of events is one of several reasons that prevent confidence in such a conclusion.
We explored the distribution of WSS events by error type, as did five other studies; however, each of those studies had notable methodological differences with our study. For example, a couple of the studies combined wrong-side and wrong-site errors into a single category,8,12 and several studies merged error type and procedure type (e.g., wrong digit, wrong organ).11,13,14 Nevertheless, a majority of the studies, like ours, found that wrong-side and wrong-site errors were more frequent than wrong-procedure and wrong-patient errors.8,12–14 In contrast, one study reported more wrong-procedure and wrong-patient errors than side and site errors, but this finding could be explained by the study using insurance claims as the data source, instead of patient safety event reports.11
Three prior studies reported that the orthopedics specialty and neurosurgery specialty were frequently associated with WSS events.5,7,11 Our findings were similar when including the spinal surgery specialty, which includes surgeons trained in orthopedics and/or neurosurgery. We found that the urology specialty was also frequently related with WSS events, and this finding is consistent with two recent studies.5,7 In contrast with the recent studies,5,7,11 the current study found that interventional radiology, anesthesia, and pain management were among the specialties most frequently associated with WSS events. It is unclear why the other recent studies had dissimilar findings, but it could be because two of the studies used insurance claims as a data
source7,11 and the third study had a relatively small WSS sample size (n=22).5
Our study examined the relation between WSS and both body region and specific body part. We identified only two recent studies6,9 that also explored the relation, and both narrowed the scope to the spine region. Similar to our findings, one study reported that the lumbar portion was most frequently associated with WSS events,9 while another study found, consistent with our results, that the thoracic portion was least frequently associated.6
The present study explored the relation between WSS and 34 categories of specific procedures, nested across 11 categories of procedure groups. Among the recent WSS studies, we identified one that reported specific spinal procedures9 and another that reported specific urological procedures.8 Unfortunately, our study of spinal procedures was not as specific as the comparison study;9 nevertheless, like in their study, a majority of our procedures were types of spinal decompression/stabilization procedures. Similarly, the recent study8 of urological procedures also used greater specificity in their categories of procedures; yet, both the comparison study and our study found that a majority of the WSS events involved endoscopy with or without a stent.
Strategies to Mitigate Risk of Wrong-Site Surgery
Since our last study,3 the Patient Safety Authority and the Pennsylvania Department of Health published Final Recommendations to Ensure Correct Surgical Procedures and Correct Nerve Blocks.18 The evidence-based recommendations cover the following perioperative topics: preoperative verification and reconciliation, site marking, time-out and intraoperative verification, and accountability. The recommendations are intended to provide a foundation of principles that, if fully implemented, should substantially reduce the likelihood of WSS. However, these recommendations are not exhaustive, and we encourage practitioners to pursue additional strategies specific to their specialty.
Limitations and Future Research
We did not calculate a rate of WSS events, due to an absence of reliable denominator data (i.e., frequency of invasive operative procedures performed). Given our lack of WSS rate, WSS being a relatively infrequent type of patient safety event, and challenges in meeting statistical test assumptions, we did not conduct statistical analyses of WSS occurrence. While our sample size of WSS event reports is noteworthy, relative to other studies, the depth of clinical details in our WSS reports was often lacking, which also prevented a study of the root causes and other clinically relevant variables (e.g., patient body mass index, patient diagnosis, surgeon experience, whether the patient had an anatomical variation, and how the error was detected).
Conclusion
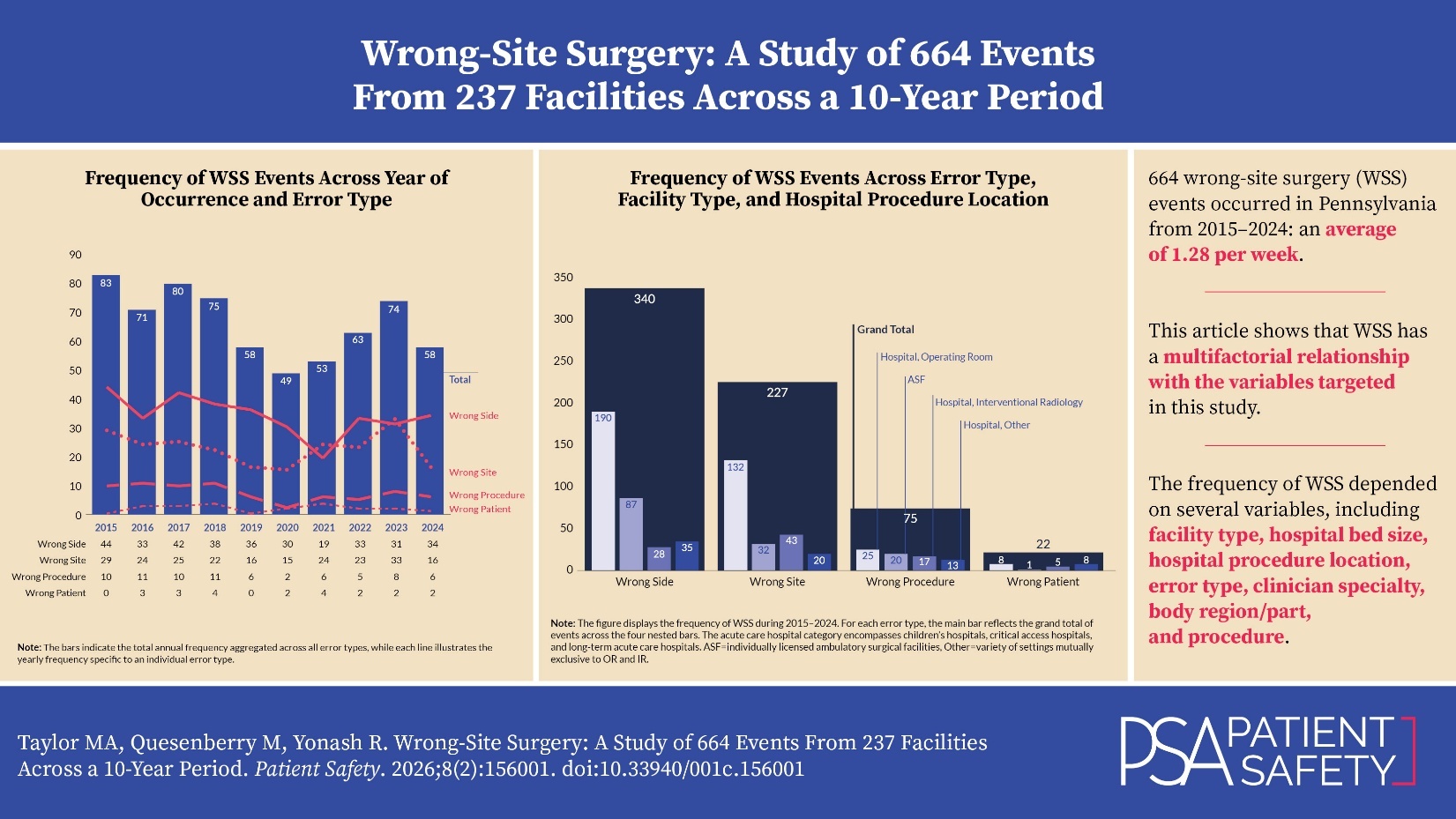
We identified 664 WSS events that occurred in Pennsylvania during the 10-year period of 2015–2024, which was an average of 1.28 per week. These “never events” were reported across 237 facilities, and our analysis revealed that the frequency of WSS was highly dependent on a range of variables, including facility type, hospital bed size, hospital procedure location, error type, clinician specialty, body region/part, and procedure. The 16 visuals (figures, tables, and appendices) in this manuscript allow for a thorough analysis that will help readers understand the extent to which WSS has a multifactorial relationship with the variables targeted in this study. Stakeholders could leverage these findings, along with other data sources (e.g., facility-specific data), to identify WSS-related factors to target and inform interventions to enhance patient safety.
Notes
This analysis was exempted from review by the Advarra Institutional Review Board.
Data used in this study cannot be made public due to their confidential nature, as outlined in the Medical Care Availability and Reduction of Error (MCARE) Act (Pennsylvania Act 13 of 2002).16
Artificial intelligence (OpenAI’s ChatGPT 4.1) was used only to improve sentence clarity. No AI was used for data analysis, interpretation, or generation of original content. The authors take full responsibility for the accuracy and integrity of the manuscript.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
Matthew A. Taylor (MattTaylor@pa.gov) is a research scientist on the Data Science & Research team at the Patient Safety Authority, where he conducts research, uses data to identify patient safety concerns and trends, and develops solutions to prevent recurrence.
Molly Quesenberry (moquesenbe@pa.gov) is a patient safety advisor with the Patient Safety Authority, serving healthcare facilities in the North Central region of Pennsylvania. Prior to joining PSA, she was a staff nurse, a director of nursing, a patient safety officer, and a director of quality and regulatory programs.
Robert A. Yonash is a registered nurse and a retired patient safety advisor. He worked at the Patient Safety Authority as an advisor during 2009 to 2024 in the Southwest region of Pennsylvania.
PA-PSRS is a secure, web-based system through which Pennsylvania hospitals, ambulatory surgical facilities, abortion facilities, and birthing centers submit reports of patient safety–related incidents and serious events in accordance with mandatory reporting laws outlined in the Medical Care Availability and Reduction of Error (MCARE) Act (Act 13 of 2002). All reports submitted through PA-PSRS are confidential and no information about individual facilities or providers is made public.
The criteria were designed to identify reports involving wrong-side or wrong-procedure errors. Reports describing wrong-side errors often reference both the left and right sides, while those involving wrong-procedure errors—particularly those related to incisions or excisions—typically mention both procedures.
Within PA-PSRS, the event reporter chooses among 168 care areas to indicate the location where an event occurred. In order to simplify our analysis, we sorted each of the care areas into higher-level care area groups.
Our previous article3 reported 368 WSS events during 2015–2019, but in rereview of the data we determined that one of the events should be excluded from our sample of WSS events, thereby reducing our sample to 367.
The Health Care Facilities Act of Jul. 19, 1979, P.L. 130, No. 48 defines ambulatory surgical facility (ASF) as “a facility or portion thereof not located upon the premises of a hospital which provides specialty or multispecialty outpatient surgical treatment. Ambulatory surgical facility does not include individual or group practice offices of private physicians or dentists, unless such offices have a distinct part used solely for outpatient surgical treatment on a regular and organized basis. For the purposes of this provision, outpatient surgical treatment means surgical treatment to patients who do not require hospitalization, but who require constant medical supervision following the surgical procedure performed.”
The hospital procedure location category labeled “operating room (OR)” included events occurring in the OR itself and also in the preoperative area, postoperative care unit, and procedure rooms (e.g., endoscopy/gastrointestinal laboratory, laser room, or dedicated anesthesia block room)
The hospital procedure location category labeled “other” included events that occurred in a variety of settings, such as radiation oncology, rehabilitation unit, short stay unit, invasive cardiology, emergency department, electrophysiology laboratory, intensive care unit, newborn nursery, and nursing care unit (including medical/surgical, neurology, and medical oncology units).