Introduction
The Pennsylvania Patient Safety Reporting System (PA-PSRS) is the largest patient safety data repository of its kind in the United States. In addition to over 5.3 million patient safety event reports from hospitals, ambulatory surgical facilities, abortion facilities, and birthing centers, the PA-PSRS database contains more than 473,000 long-term care (LTC) healthcare-associated infection (HAI) reports submitted from 2009 through 2025, the most recent year included in this analysis.
Methods
The LTC data from PA-PSRS[1];1 were extracted on March 1, 2026, to allow time for users to complete the entry of all 2025 resident and device utilization days, which are used for calculating rates. Report counts are based on the submission date, while overall infection rates are calculated per 1,000 resident days using the infection confirmation date to align infections with the period in which resident days occurred. Rates for infections associated with urinary catheters and central lines are calculated per 1,000 urinary catheter days or 1,000 central line days, respectively. A report is included in rate calculations if resident and/or device days were entered in PA-PSRS for the corresponding month and care area. Unless otherwise stated, statistical tests are conducted at a 0.05 significance level.
Results
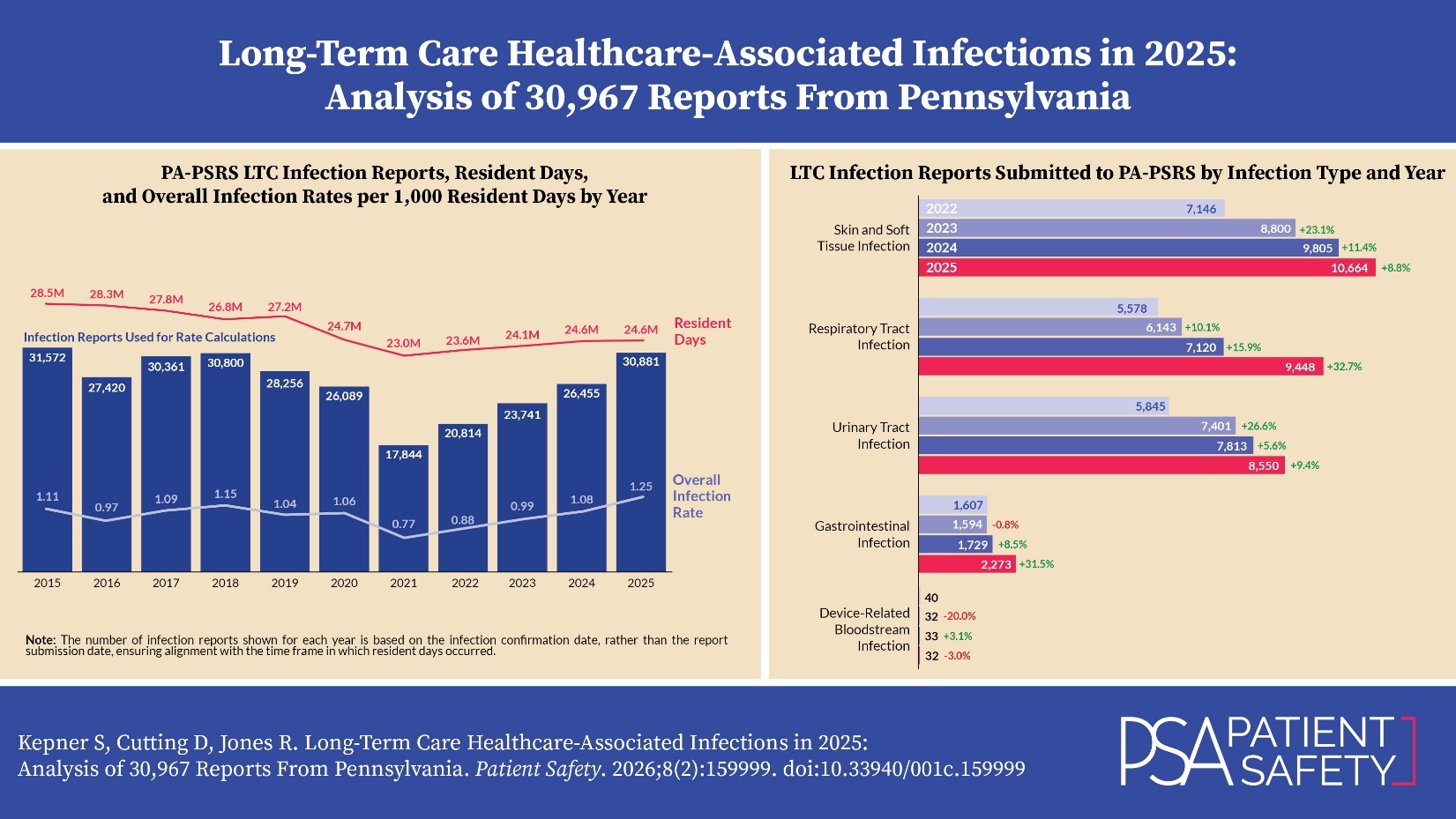
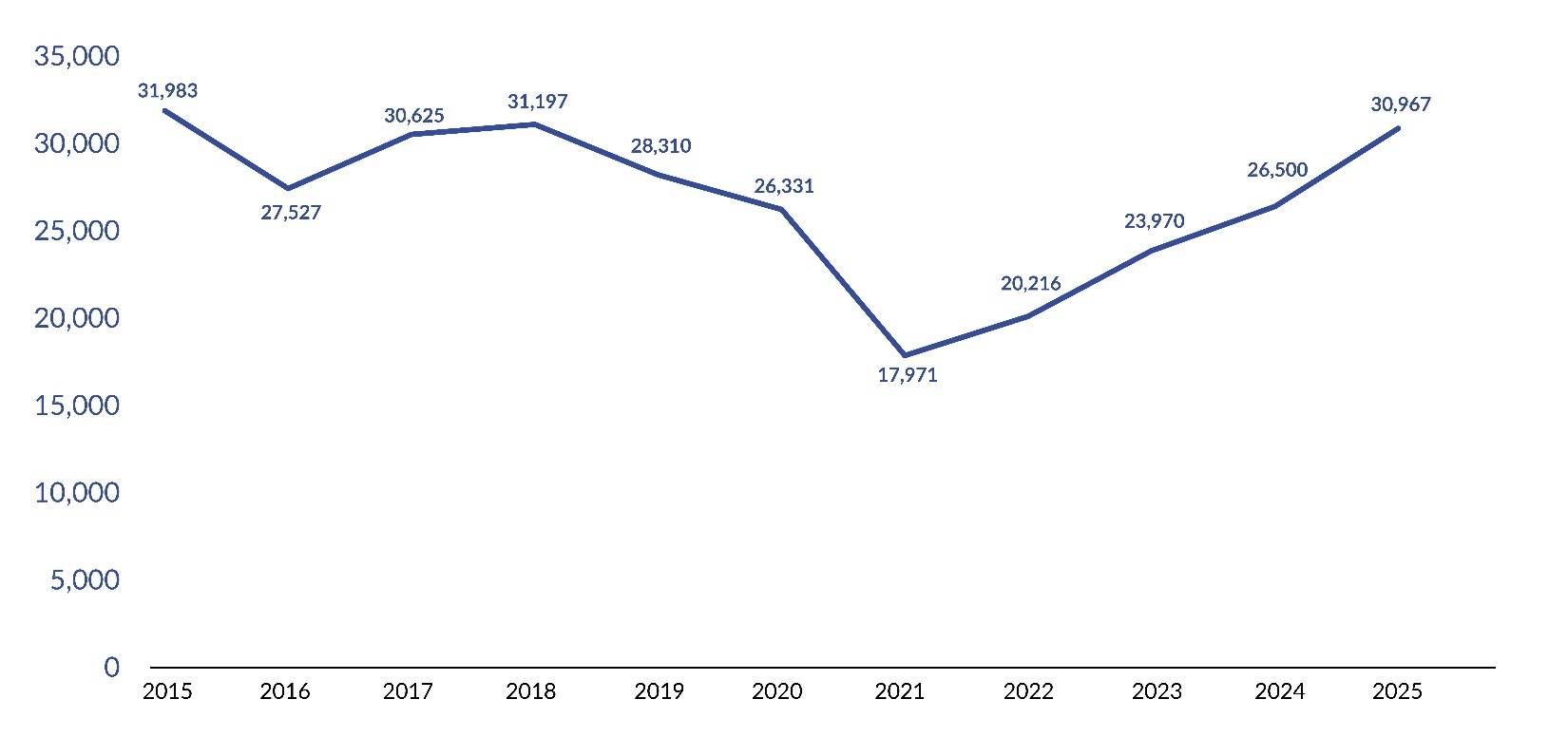
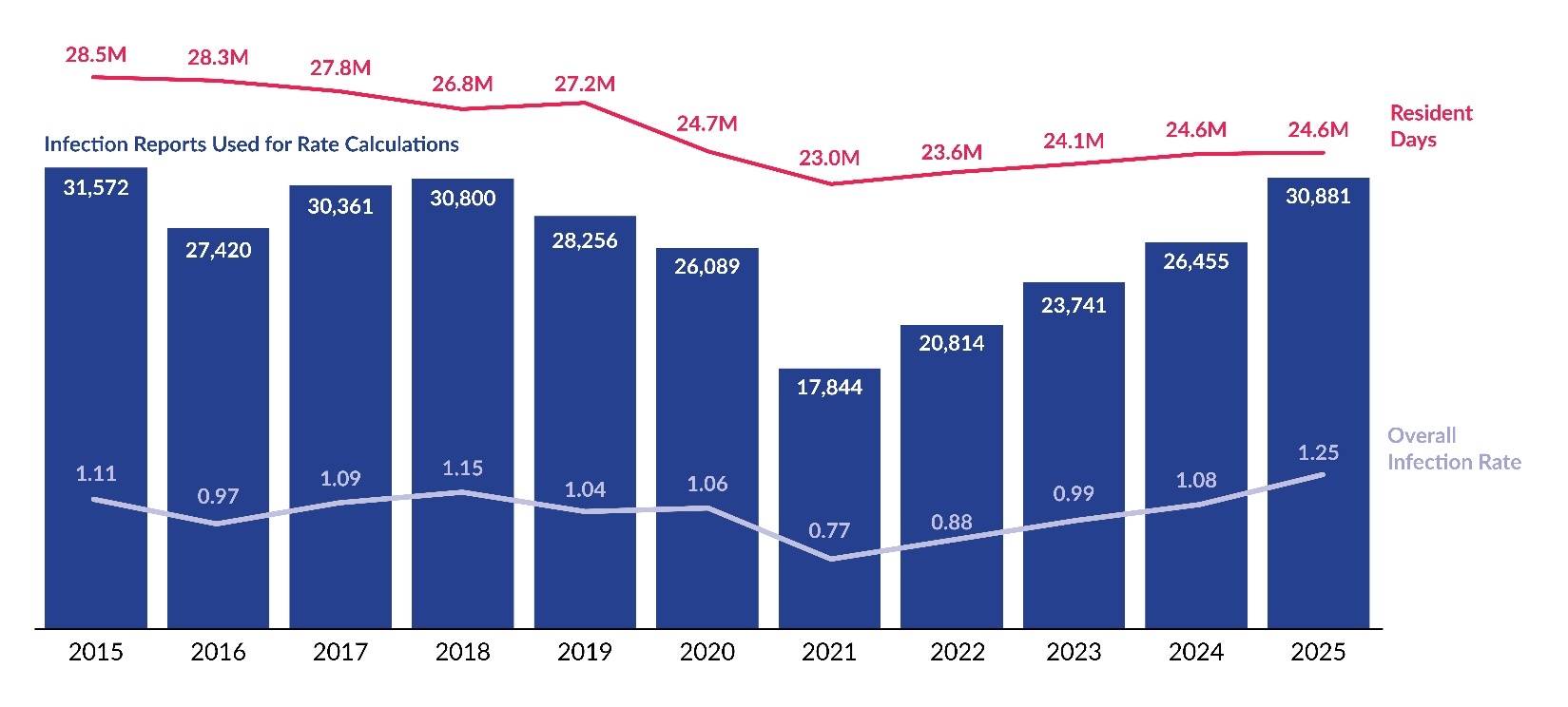
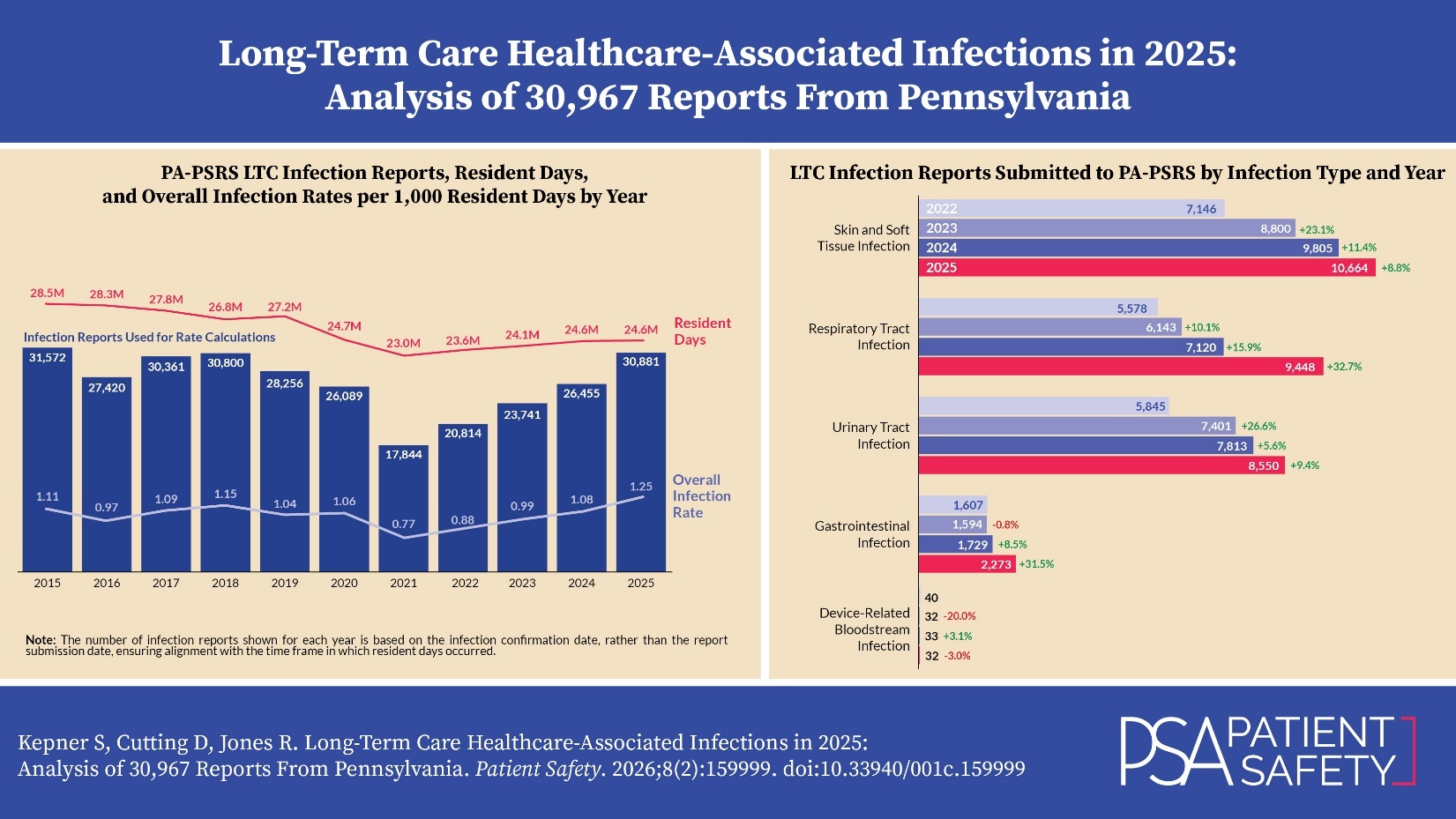
Pennsylvania’s LTC facilities submitted 30,967 infection reports to PA-PSRS in 2025, a 16.9% increase over the prior year and the fourth consecutive annual increase, with all four increases exceeding 10% (see Figure 1). As shown in Figure 2, the overall infection rate in 2025 was 1.25 infections per 1,000 resident days, representing a 15.7% increase from 2024. The 2025 rate also established a significant four-year increasing linear trend since the low point of 0.77 in 2021 (R2=0.989, p=0.0005).
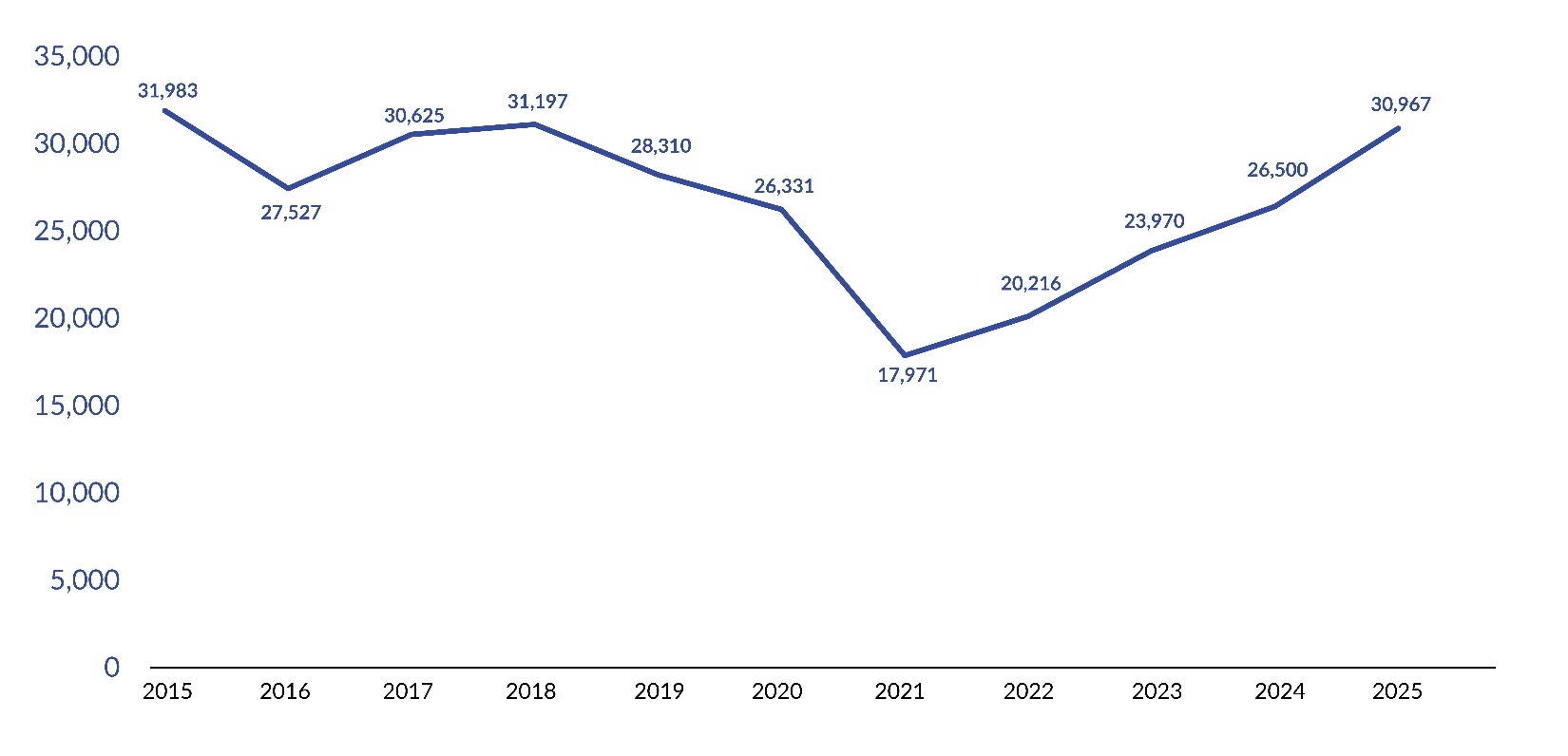
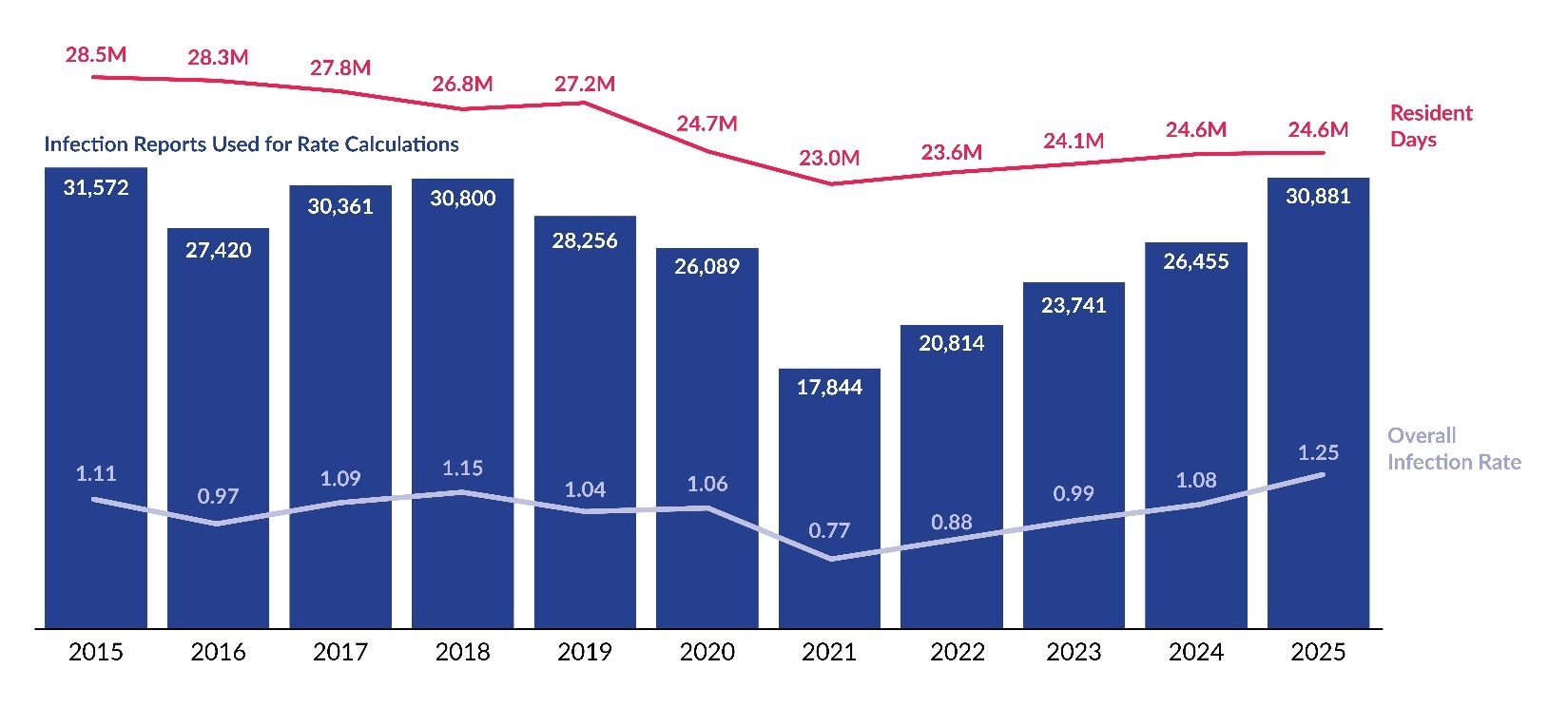
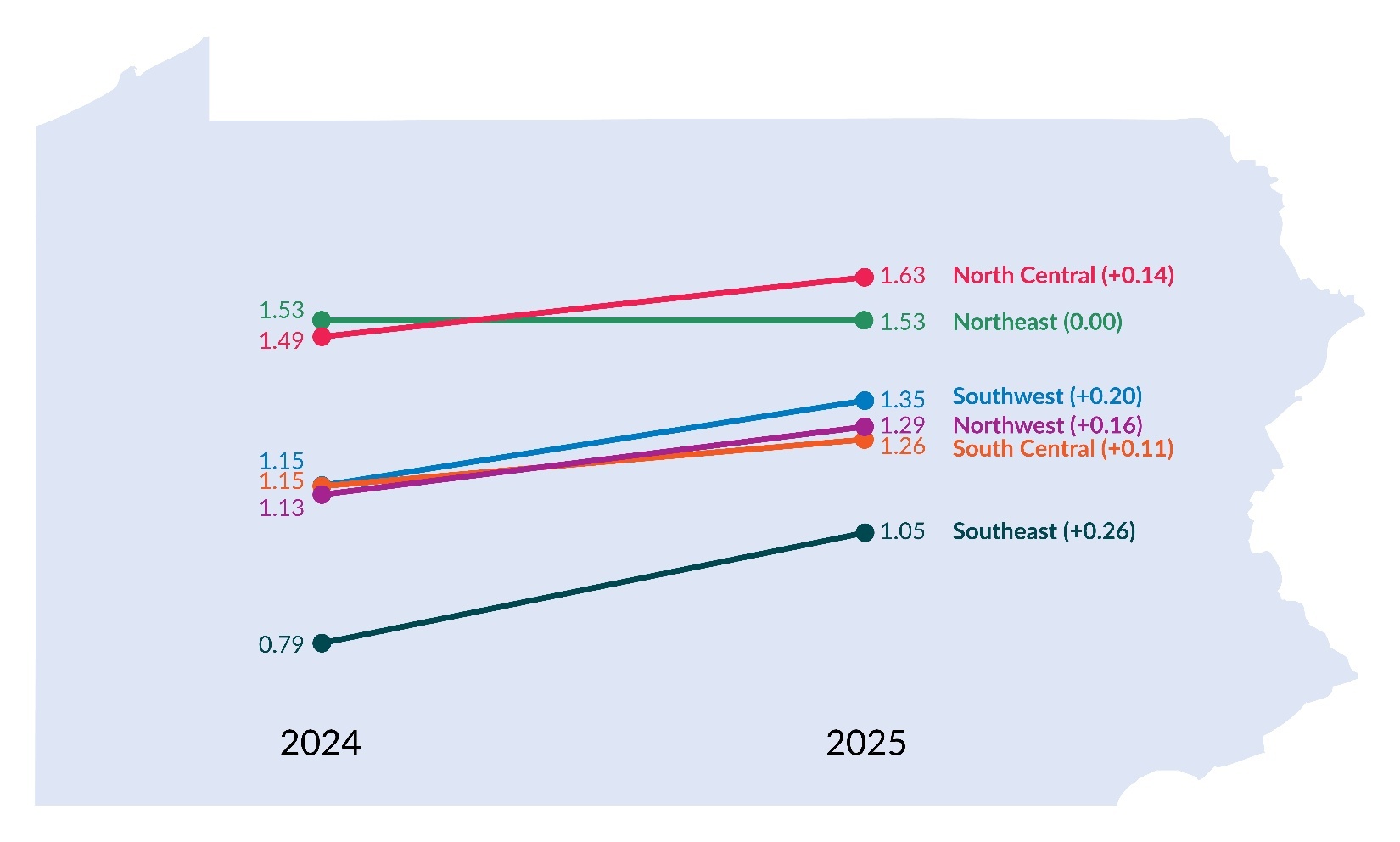
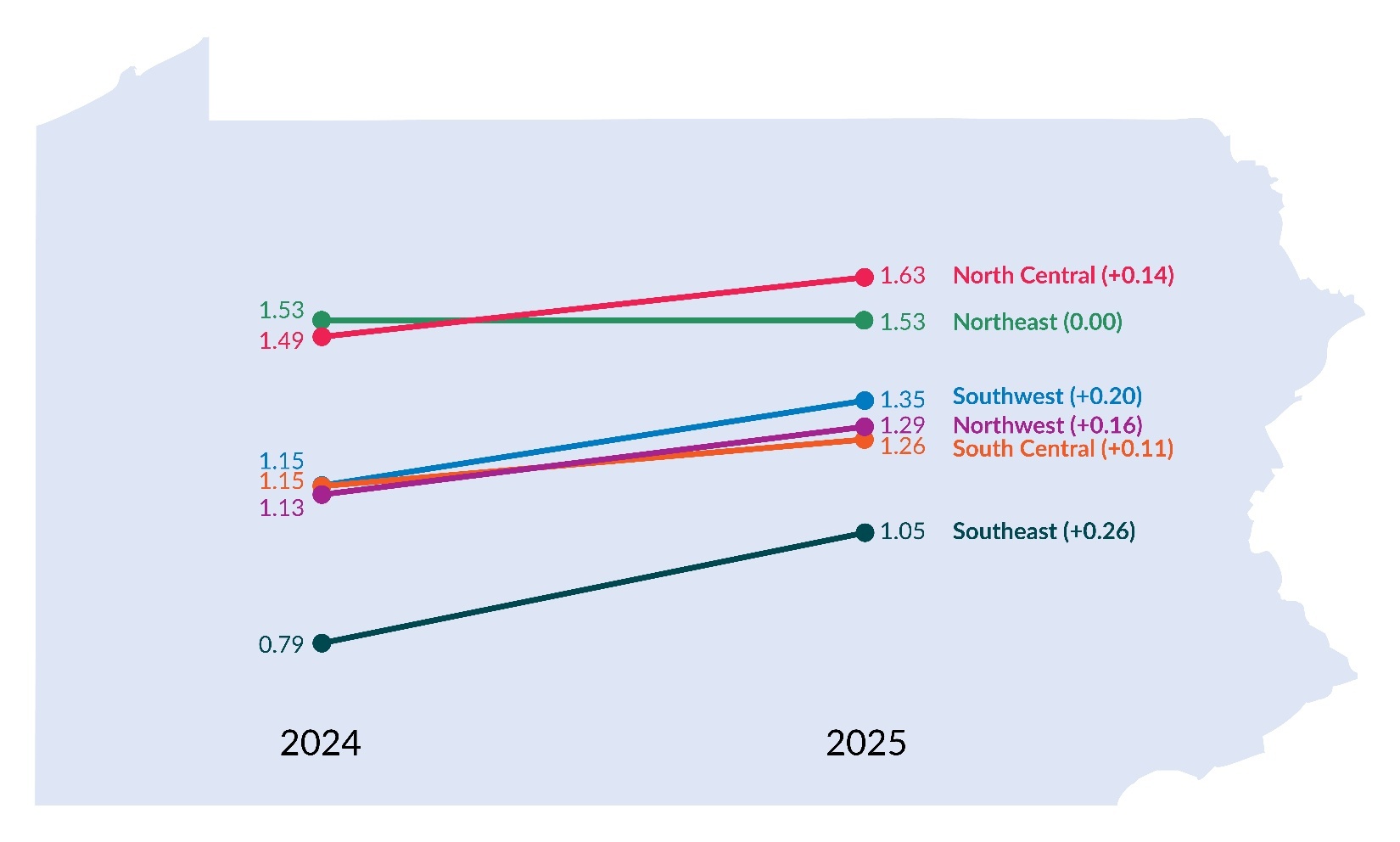
Figure 3, which displays infection rates by region, shows that infection rates increased from 2024 to 2025 across all regions of the state, except for the Northeast, which remained at 1.53. The North Central region had the highest infection rate in 2025, at 1.63 reports per 1,000 resident days, whereas the Southeast region had the lowest rate at 1.05. Although the Southeast rate remained the lowest of all regions in 2025, it showed the largest increase, rising by 0.26 points (32.9%) from 2024 to 2025. The distribution of LTC infection reports and infection rates by region is shown in Table 1.
LTC Healthcare-Associated Infection Types and Subtypes
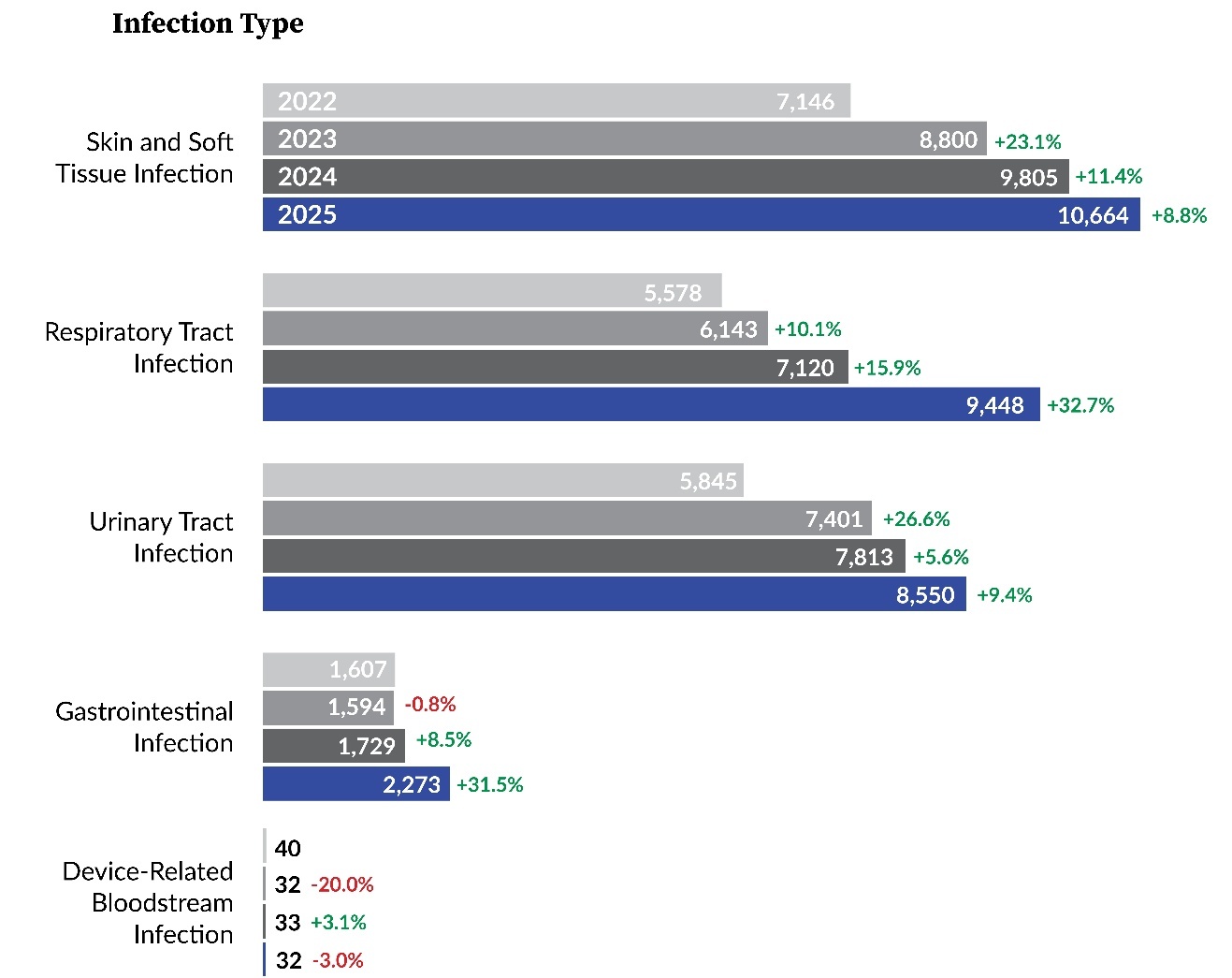
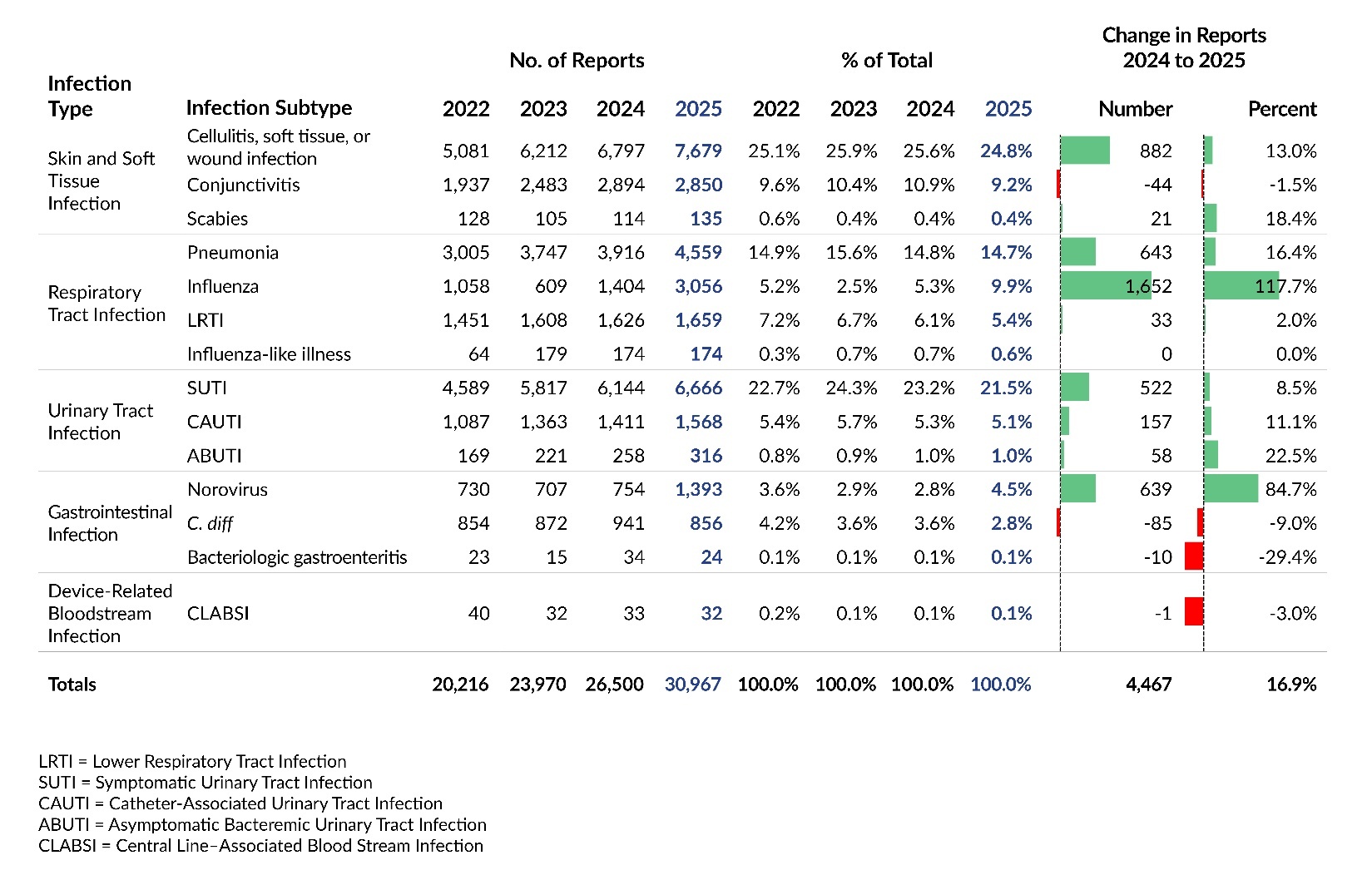
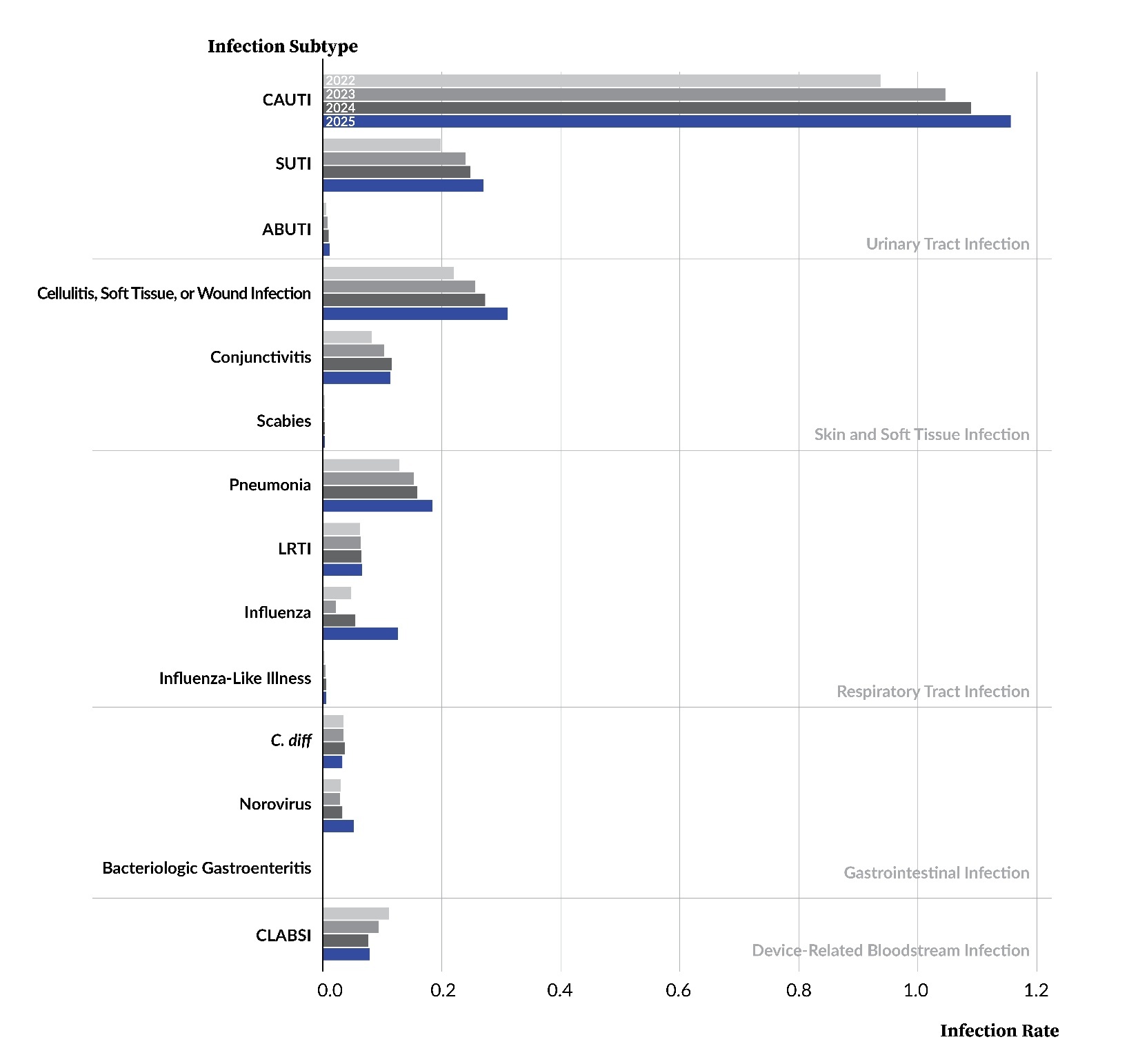
LTC facility reports submitted to PA-PSRS are classified into five main infection types (Figure 4), each further divided into specific subtypes (Table 2). Figure 4 and Table 2 show the distribution of reports across infection types and subtypes, respectively, for the past four years. Across this period, skin and soft tissue infections (SSTIs) have been the most frequently reported type, reflecting the predominance of the cellulitis, soft tissue, or wound infection subtype. Symptomatic urinary tract infection (SUTI) and pneumonia were also among the most frequently reported subtypes throughout the four-year period.
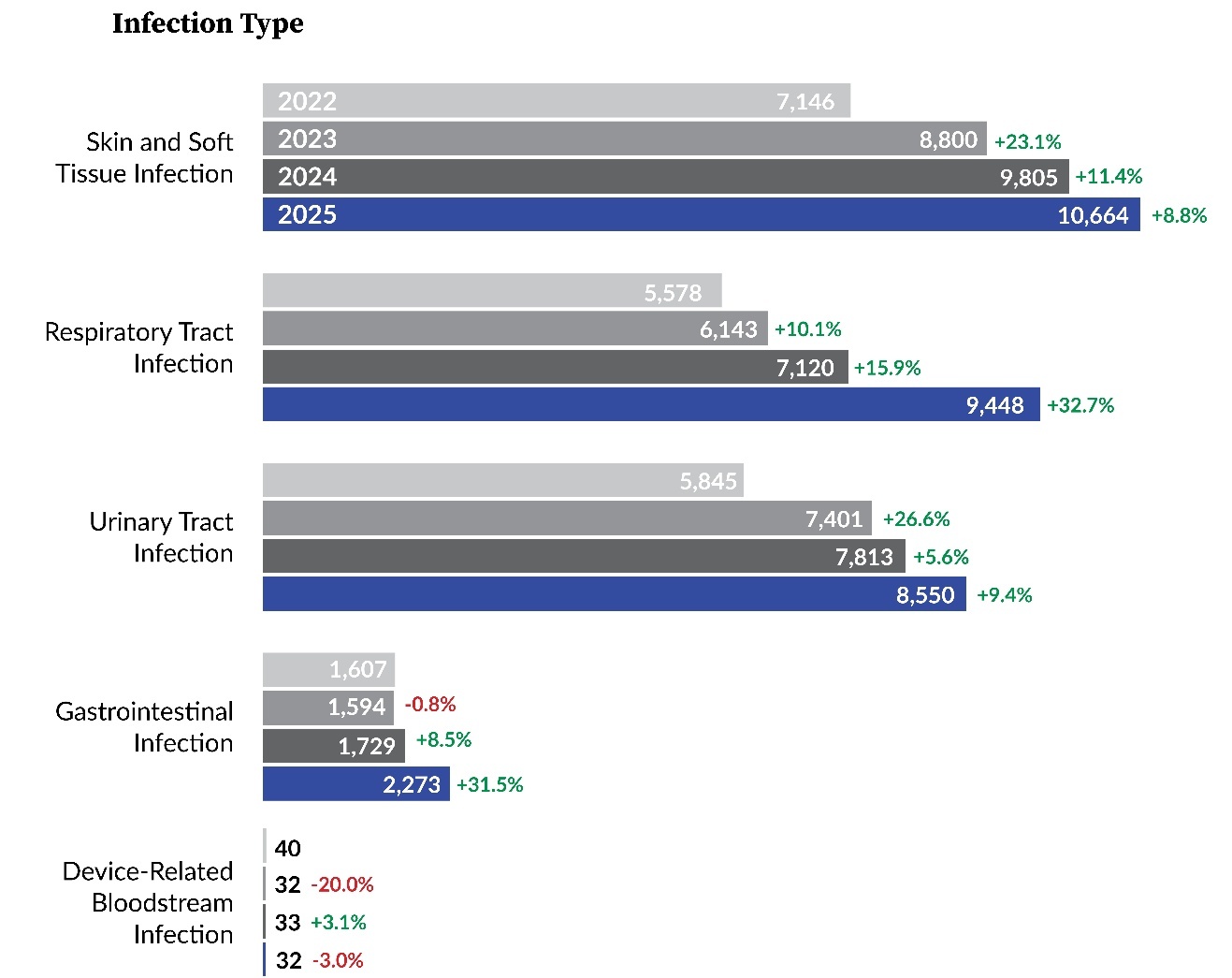
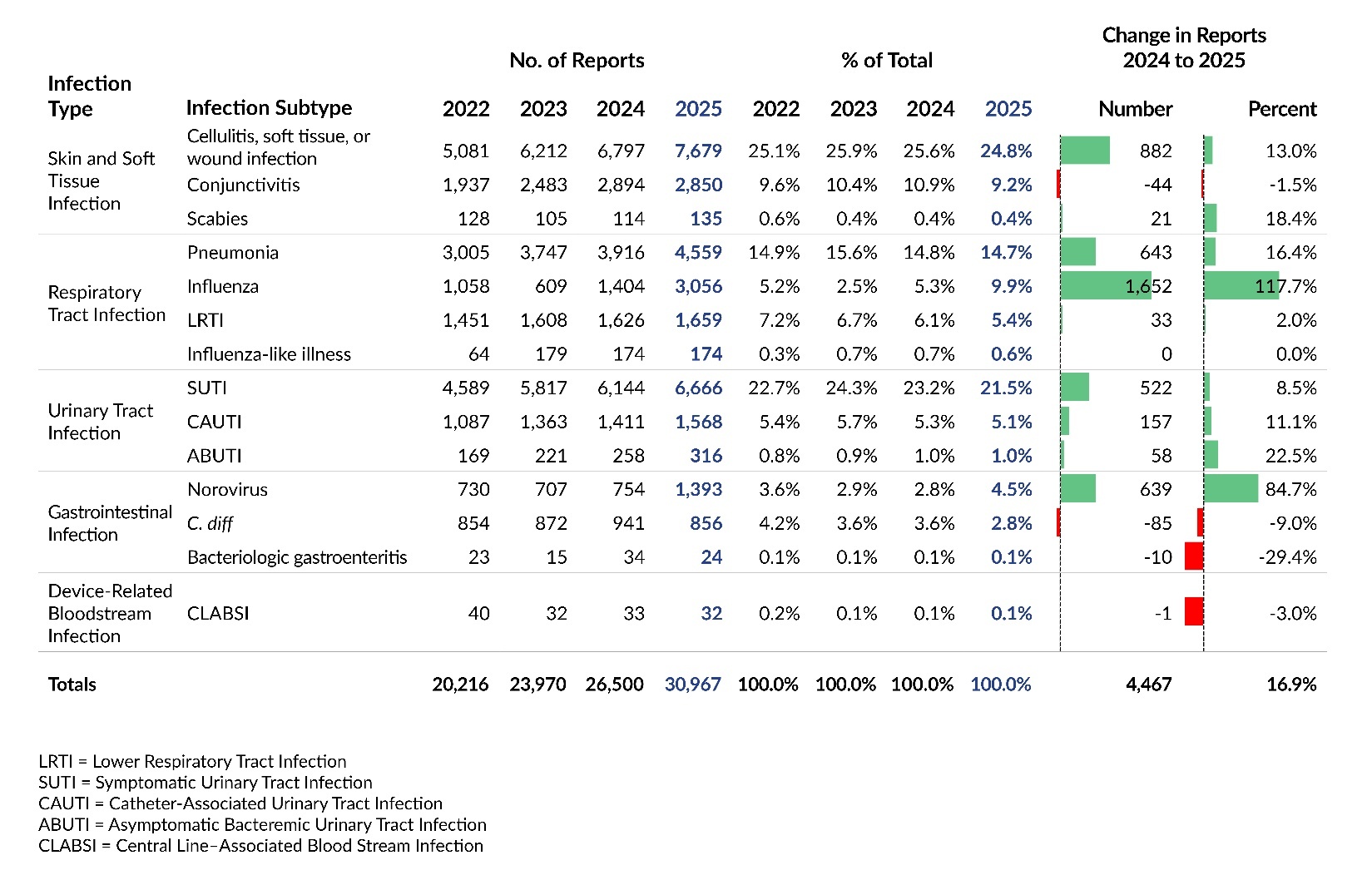
In 2025, respiratory tract infections (RTIs) showed the largest increase in both number and percentage, moving from the third to the second most frequently reported infection type after three consecutive years behind urinary tract infections. This shift was driven largely by influenza, which showed the greatest increase among all subtypes, rising by 1,652 reports (117.7%). Gastrointestinal infections also showed a large percentage increase in 2025 (31.5%), largely reflecting an 84.7% increase in norovirus reports.
Care Area
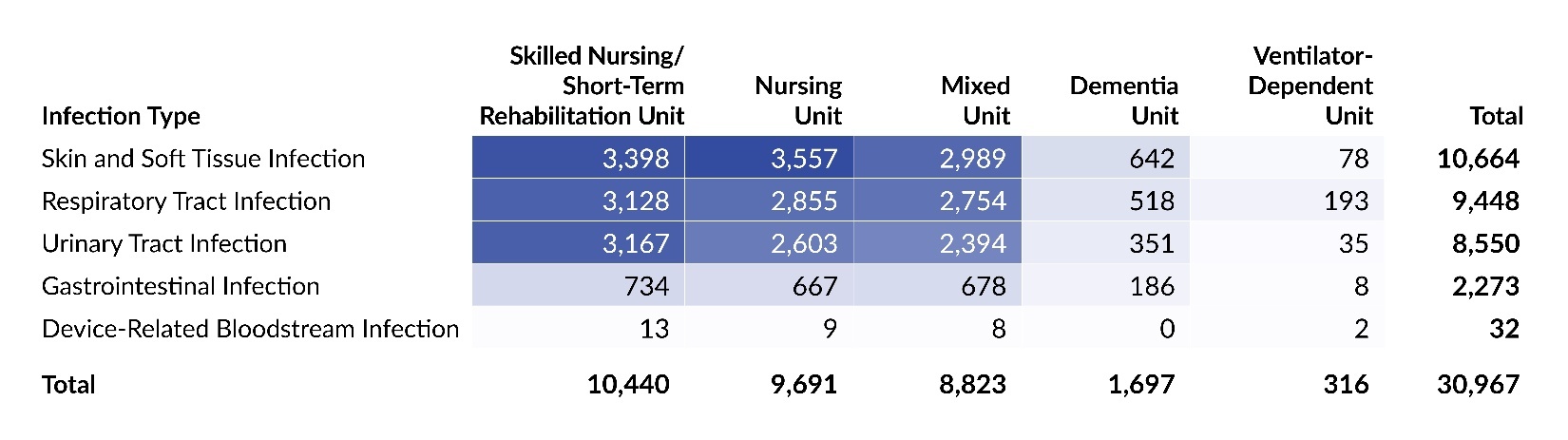
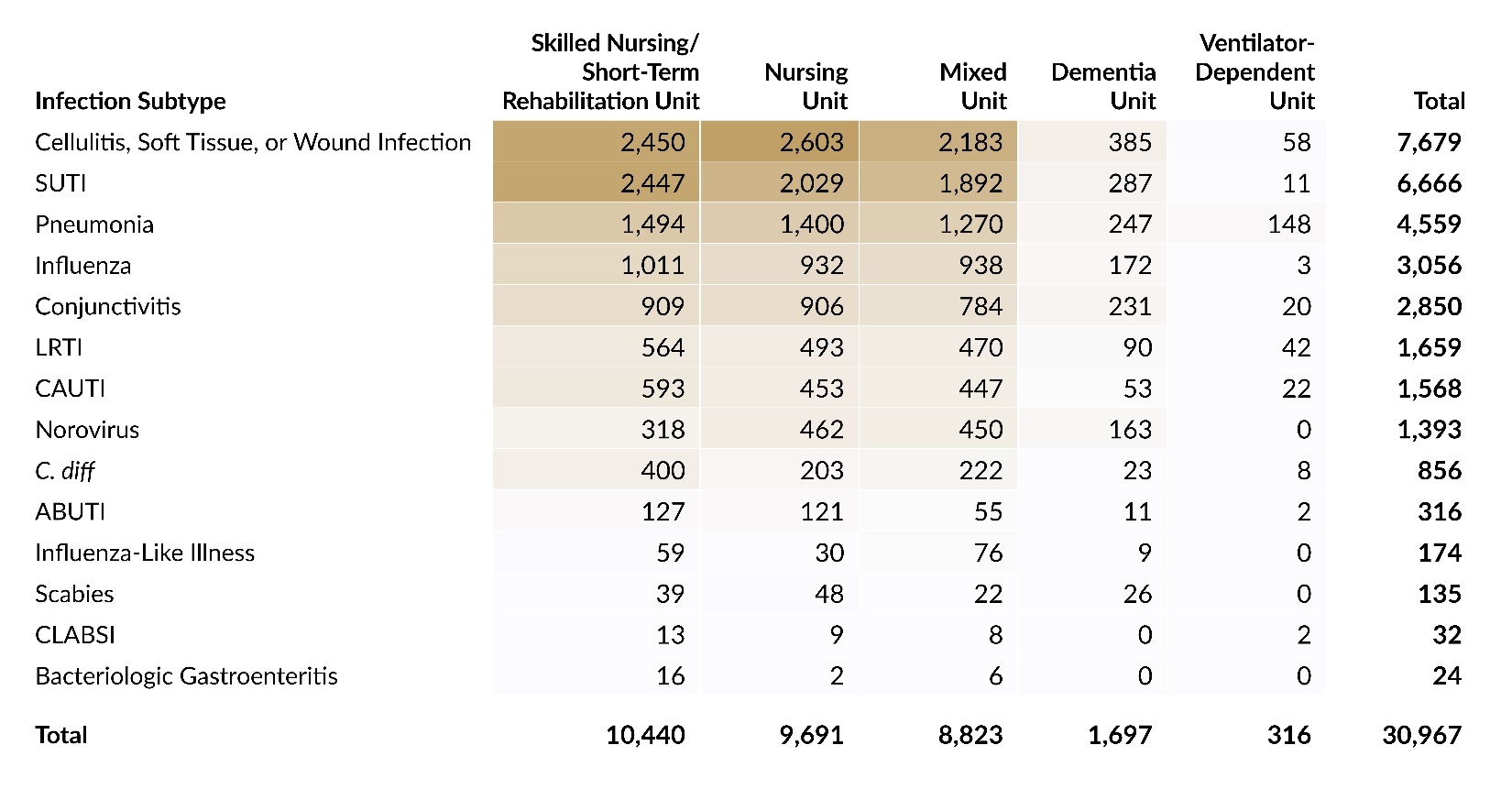
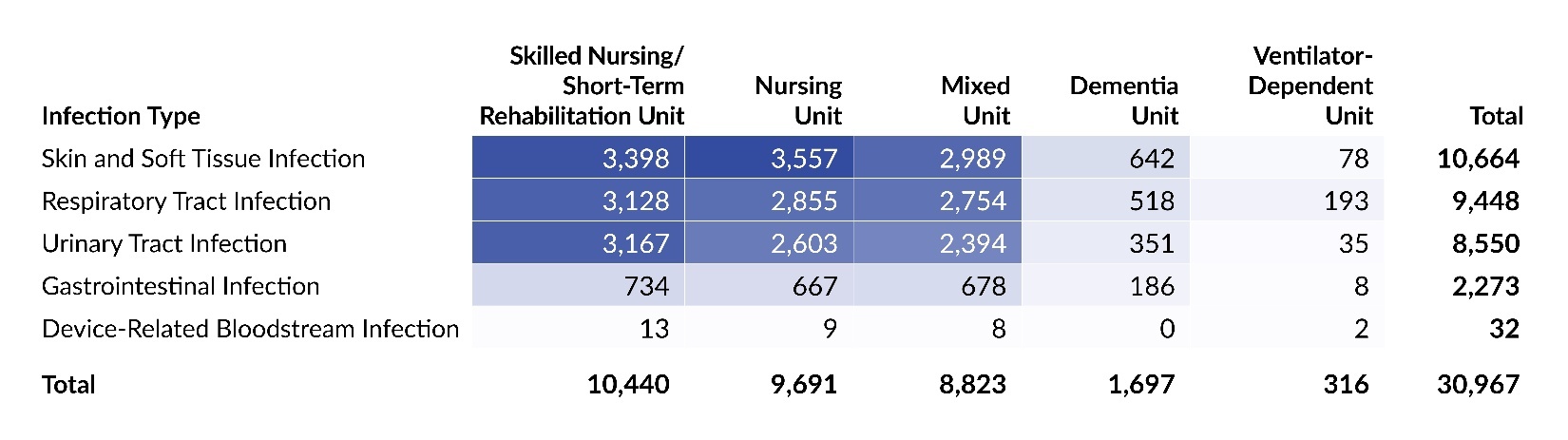
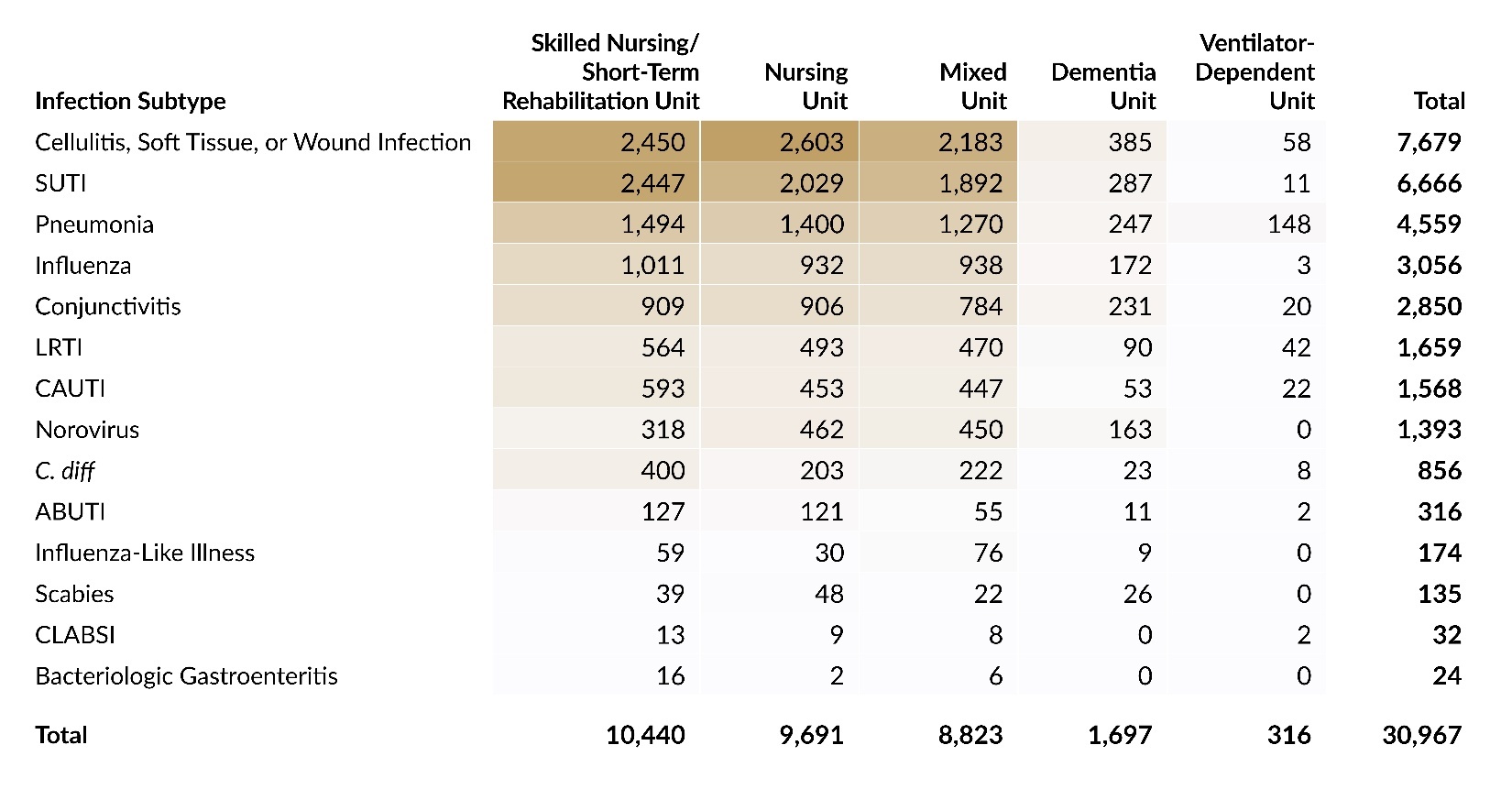
Table 3 presents the distribution of reports submitted in 2025 by infection type and care area, and Table 4 shows the corresponding distribution by infection subtype. Skilled nursing/short-term rehabilitation units accounted for one-third of all infection reports (33.7%; 10,440 of 30,967). Across care areas, SSTIs were the most reported infection type, except in ventilator-dependent units, where RTIs comprised 61.1% (193 of 316) of all reports. At the subtype level, the largest concentration of reports was seen with cellulitis, soft tissue, or wound infection in skilled nursing/short-term rehabilitation units. The highest proportion observed for any infection subtype in any care area was in ventilator-dependent units, where pneumonia reports accounted for 46.8% (148 of 316) of all reports.
LTC Healthcare-Associated Infection Rates
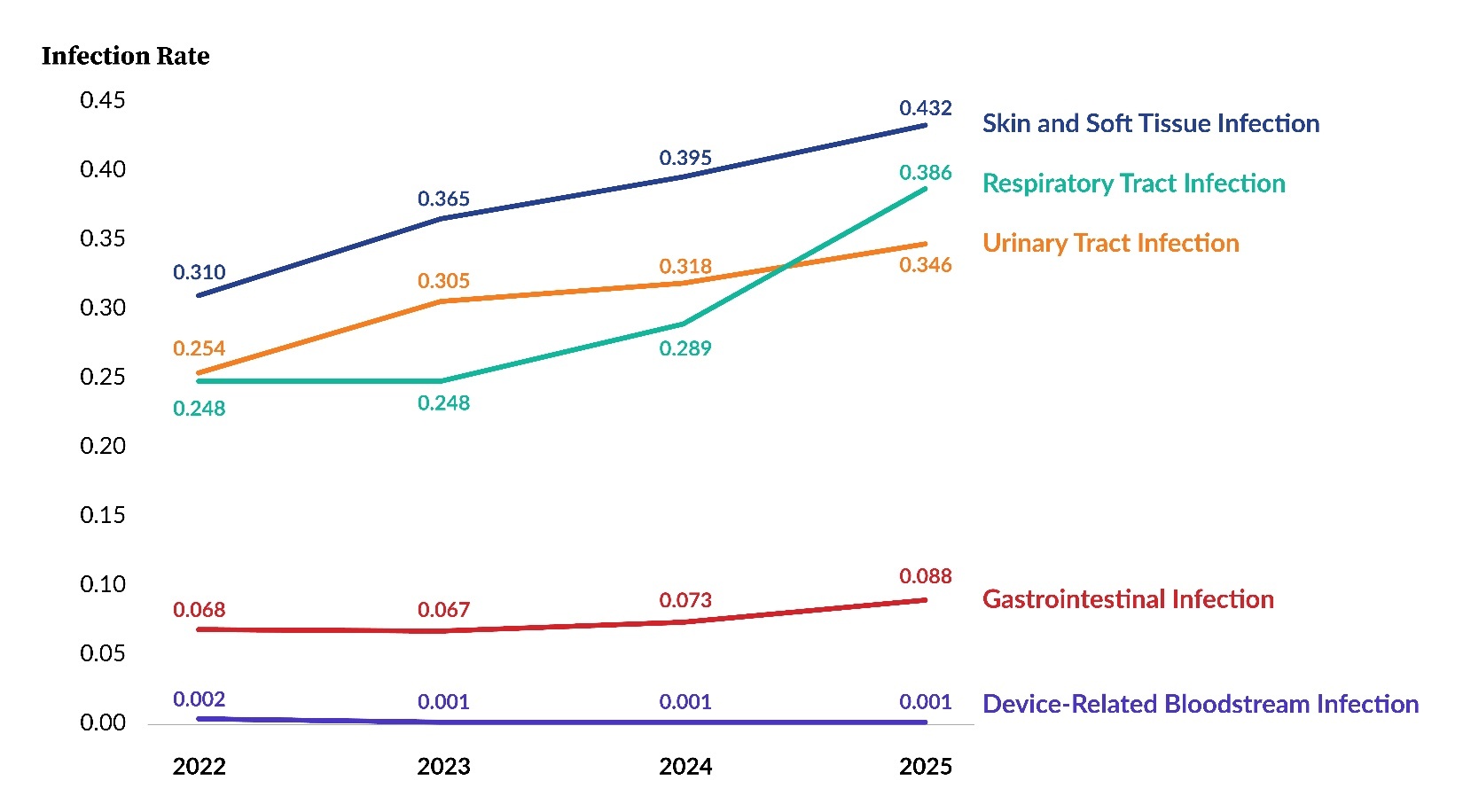
Figure 5 shows rates per 1,000 resident days for the five main infection types for 2022 through 2025. The overall infection rate increased from 1.08 in 2024 to 1.25 in 2025 due to rising rates across all infection types, except for device-related bloodstream infections, which essentially remained the same. Of note is the comparatively higher slope exhibited by the Respiratory Tract Infection line among the segments going from 2024 to 2025 and how it intersects with the Urinary Tract Infection line.
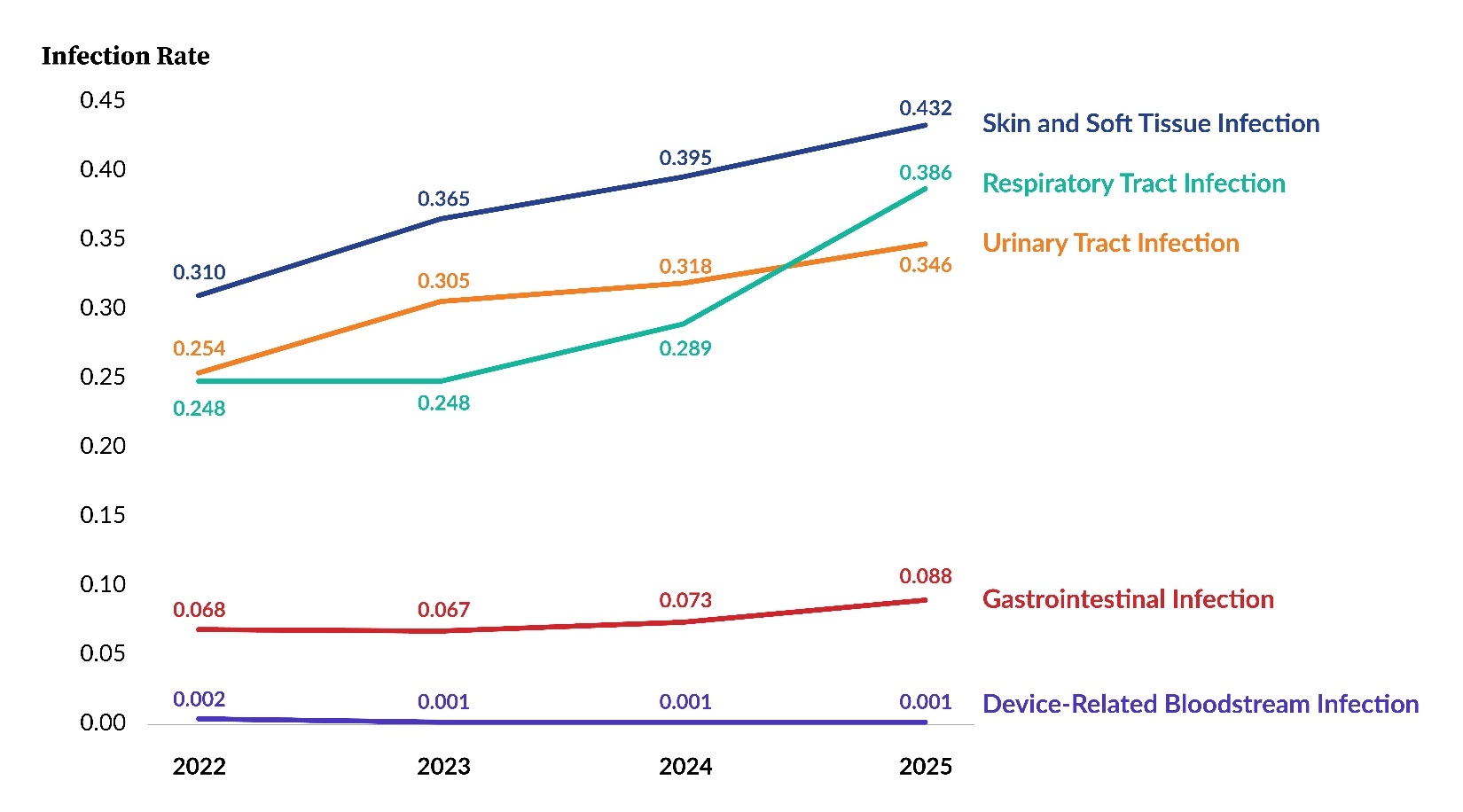
Figure 6 and Table 5 display rates for each infection subtype from 2022 through 2025. The influenza infection subtype saw the largest increase from 2024 to 2025, rising from 0.056 to 0.127 reports per 1,000 resident days, a 126.8% increase. Conjunctivitis and C. diff were the only infection subtypes that showed a decrease in rate from 2024 to 2025.
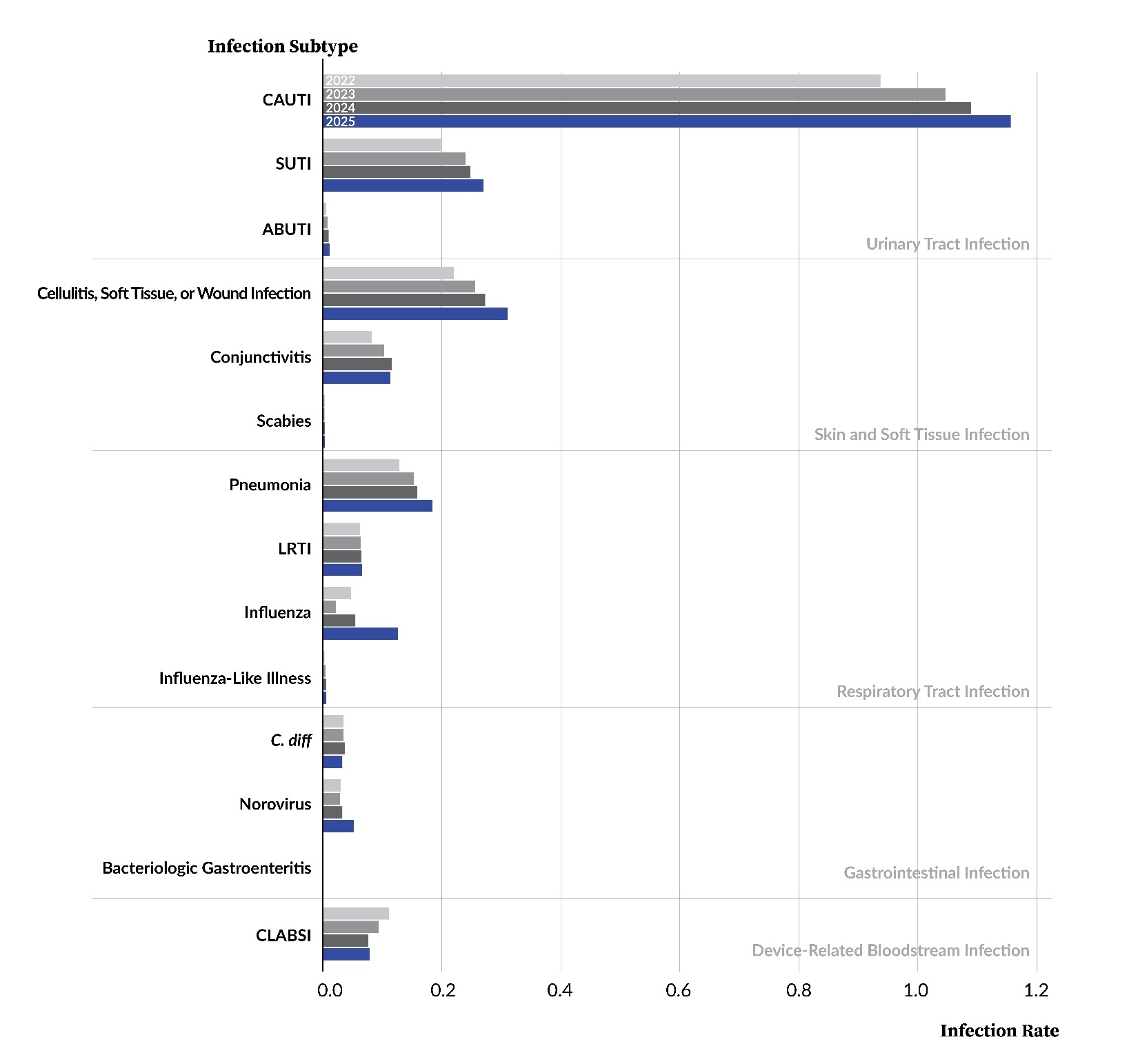
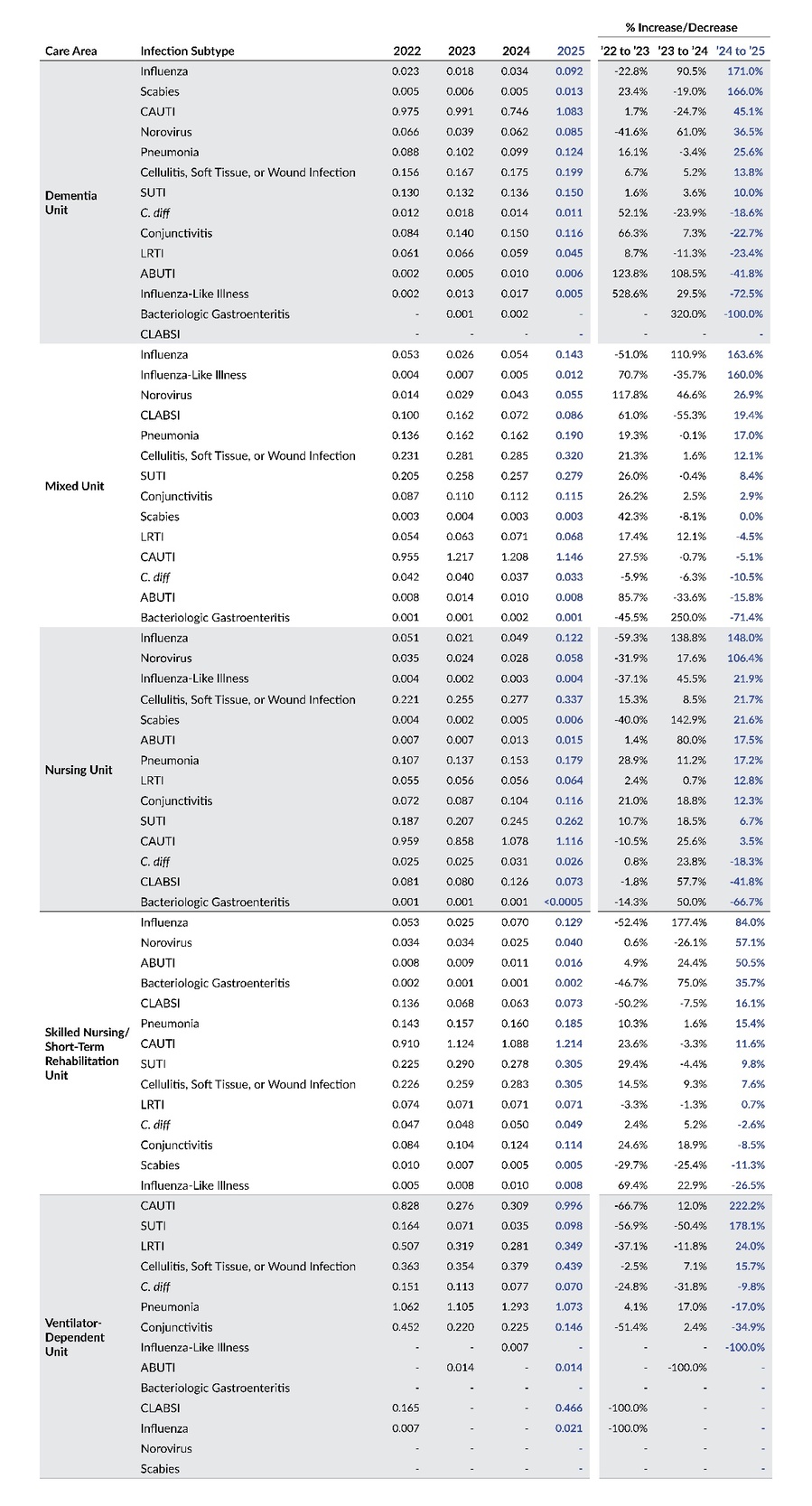
Table 6 displays infection rates by year based on care area and infection subtype. From 2024 to 2025, rates increased across all care areas for both influenza and norovirus, with the exception of ventilator-dependent units. C. diff was the only infection subtype to show a decrease in rates across all five care areas.

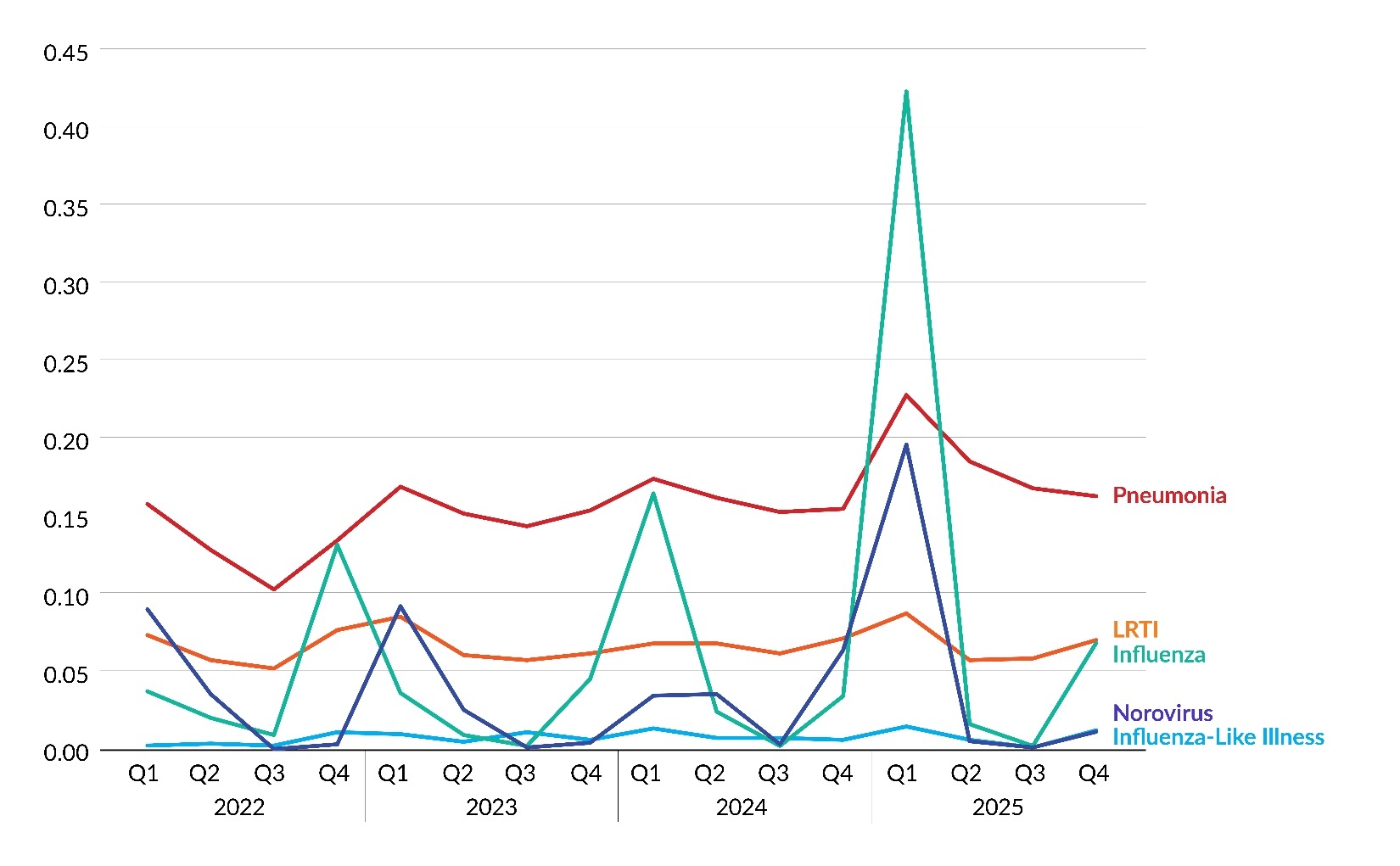
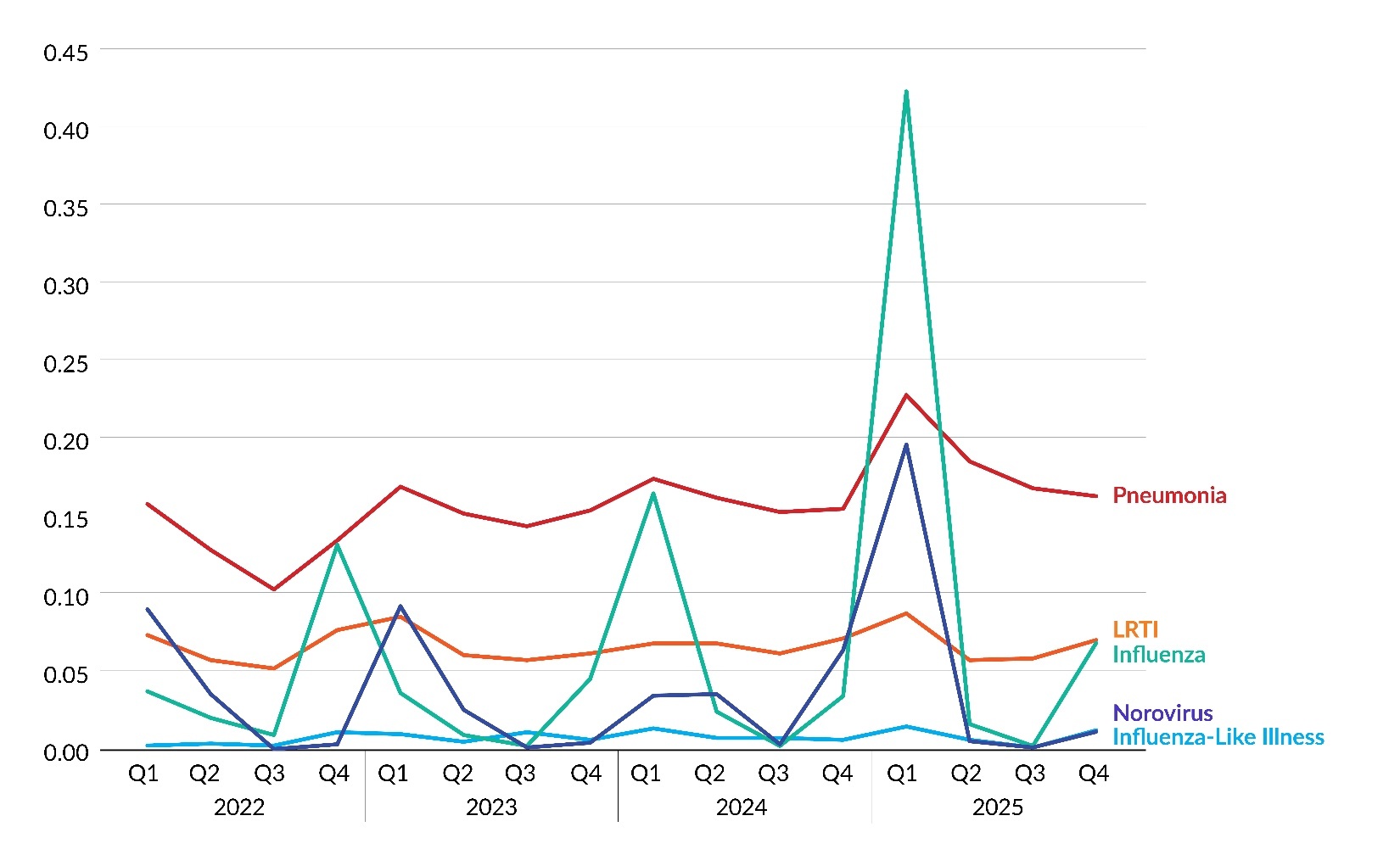
Figure 7 and Table 7 display infection rates for seasonal infection subtypes (i.e., influenza, influenza-like illness, lower respiratory tract infection [LRTI], norovirus, and pneumonia) by quarter from 2022 through 2025. These rates are calculated as the number of infections by quarter per 1,000 resident days. The rates for influenza and norovirus had a sizable jump in Q1 2025, but the percentage increase for influenza was several orders of magnitude larger than the percentage increase for norovirus—i.e., a 1,141% increase for influenza from Q4 2024 to Q1 2025 compared to a 208% increase for norovirus.
Discussion
In 2025, Pennsylvania’s LTC facilities submitted 30,967 infection reports to PA-PSRS and recorded 24.6 million resident days, with an overall infection rate of 1.25 per 1,000 resident days based on eligible reports. This marks a 16.9% increase in total infection reports and a 15.7% rise in the infection rate compared to 2024. Notably, 2025 represents the fourth consecutive annual increase, with the rate rising from 0.77 in 2021 to 1.25 in 2025.
The overall infection rate increased due to rising rates across all infection types except for device-related bloodstream infections. Notably, higher rates of influenza and norovirus were reported in 2025, with a Q1 peak that aligns with expected seasonal patterns but is more pronounced than in prior years. The increase in influenza reporting is consistent with PA-NEDSS (Pennsylvania’s version of the National Electronic Disease Surveillance System) data for the same period.2 In addition, the Pennsylvania Department of Health updated guidance for LTC facilities in November 2024 to encourage influenza testing among residents with respiratory symptoms,3 which may have contributed to increased reporting. Norovirus is highly contagious, easily spread within LTC settings, and capable of causing infection at very low doses.4
These findings underscore the importance of the Patient Safety Authority’s (PSA’s) ongoing efforts to provide LTC facilities with education and resources for surveillance, reporting, and infection prevention. In 2025, PSA infection prevention advisors continued their work with infection preventionists and facility leaders, offering expanded opportunities for support and guidance. Infection Prevention Office Hours were introduced as a monthly forum for facilities to ask questions related to surveillance and reporting. Advisors also broadened educational outreach by providing training sessions on HAI surveillance and reporting, along with biannual modules reviewing Medical Care Availability and Reduction of Error (MCARE) requirements and HAI surveillance criteria.
Conclusion
In 2025, there was a rise in both the number of infection reports submitted to PA-PSRS and the overall infection rate across Pennsylvania’s LTC facilities. The increase in overall rate in 2025 was driven by increases in the rates of all infection types except for device-related bloodstream infections, with respiratory tract infections, particularly influenza, showing the most substantial increase in both number and rate.
Notes
This analysis was exempted from review by the Advarra Institutional Review Board.
Data used in this study cannot be made public due to their confidential nature, as outlined in the Medical Care Availability and Reduction of Error (MCARE) Act (Pennsylvania Act 52 of 2007).
Artificial intelligence (Microsoft Copilot) was used only to improve sentence clarity. No AI was used for data analysis, interpretation, or generation of original content. The authors take full responsibility for the accuracy and integrity of the manuscript.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
Shawn Kepner (shawkepner@pa.gov) is a data scientist at the Patient Safety Authority (PSA). He is responsible for providing actionable insights using data science techniques and works with staff to focus resources and research in areas that have the greatest benefit to patient safety. He also serves as the data editor for Patient Safety, PSA’s award-winning, peer-reviewed journal.
Denise Cutting is a registered nurse and infection prevention advisor at the Patient Safety Authority. In this role, she serves as a resource for Pennsylvania facilities through education and the development of infection prevention initiatives. She is board-certified in infection control and epidemiology (CIC).
Rebecca Jones, director of Data Science & Research for the Patient Safety Authority, leads a multidisciplinary team advancing patient safety through research that informs improvements in healthcare systems and delivers insights that bridge the gap between evidence and real-world practice. A registered nurse with a Master of Business Administration in healthcare management and certifications in patient safety, human factors, and risk management, she brings clinical experience, analytical expertise, and systems thinking to complex challenges. She has authored more than 40 peer-reviewed publications and contributed to national patient safety efforts with organizations such as the Institute for Healthcare Improvement, the National Quality Forum, and the Society to Improve Diagnosis in Medicine.
PA-PSRS is a secure, web-based system through which Pennsylvania long-term care facilities submit reports of healthcare-associated infections in accordance with mandatory reporting laws outlined in the Medical Care Availability and Reduction of Error (MCARE) Act (Act 52 of 2007). All reports submitted through PA-PSRS are confidential and no information about individual facilities or providers is made public.