In Pennsylvania, licensed healthcare facilities are required to report all events that cause harm or have the potential to cause harm to a patient.1 The reports are captured in the Pennsylvania Patient Safety Reporting System (PA-PSRS) and then the Patient Safety Authority (PSA) analyzes them to identify causes or trends and share strategies to prevent harm. With over 5.8 million reports dating back to 2004, PA-PSRS is one of the largest data repositories of its kind in the world.2
Each year, PSA publishes an analysis of the acute and ambulatory care reports submitted to PA-PSRS, and this article expands on that work by highlighting the serious events[1];1 reported to PA-PSRS with the Medication Error event type in 2025.2
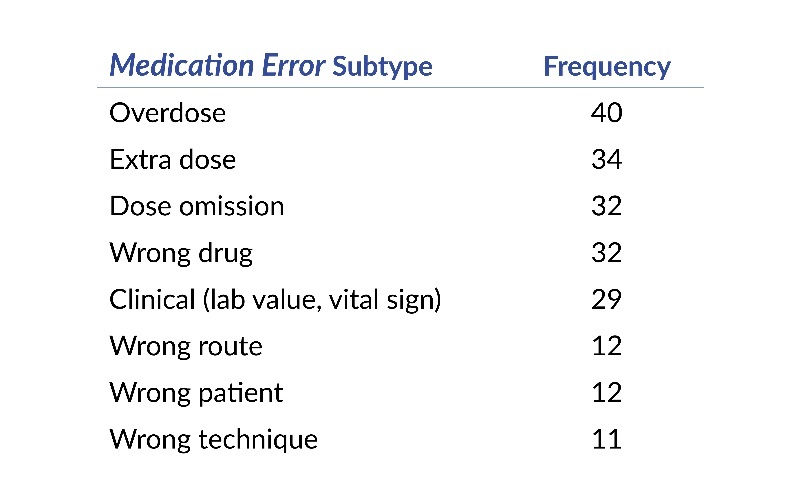
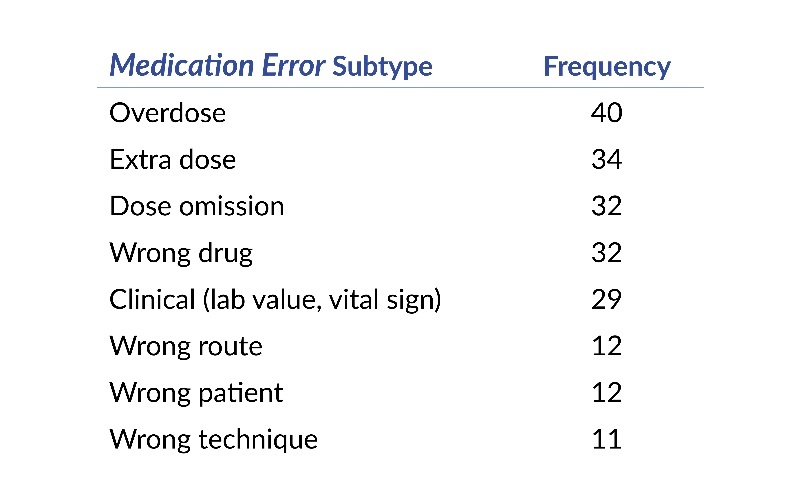
Medication Error Subtypes
In 2025, 82 facilities submitted a total of 303 serious Medication Error events to PA-PSRS. The most frequently reported Medication Error subtypes during this time frame are shown in Table 1.
High-Alert Medications
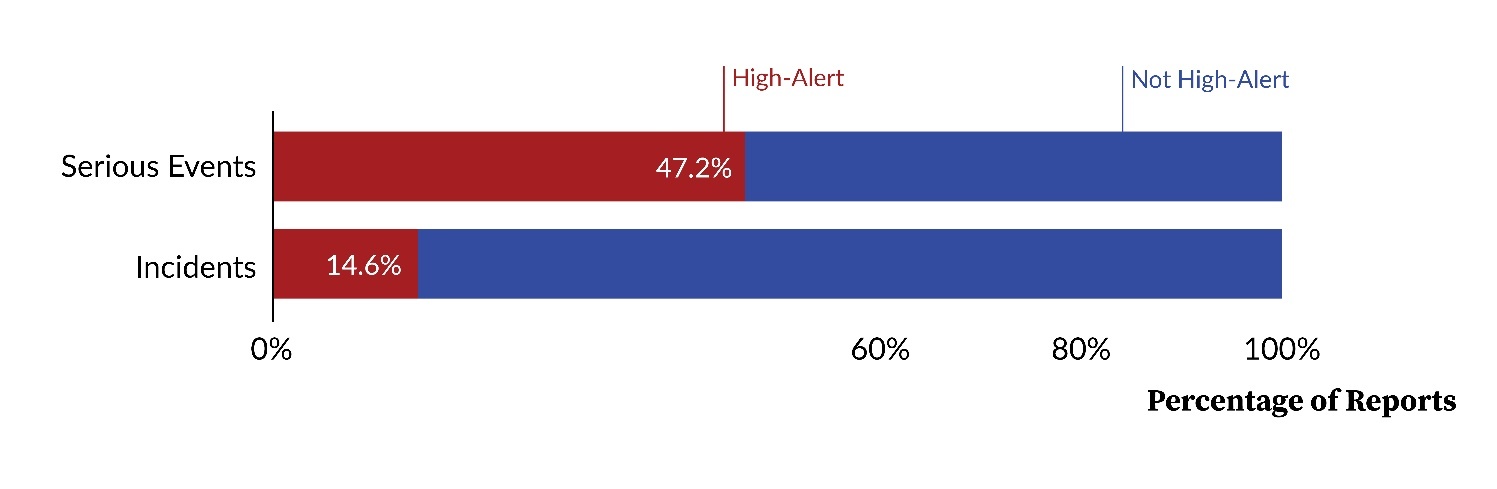
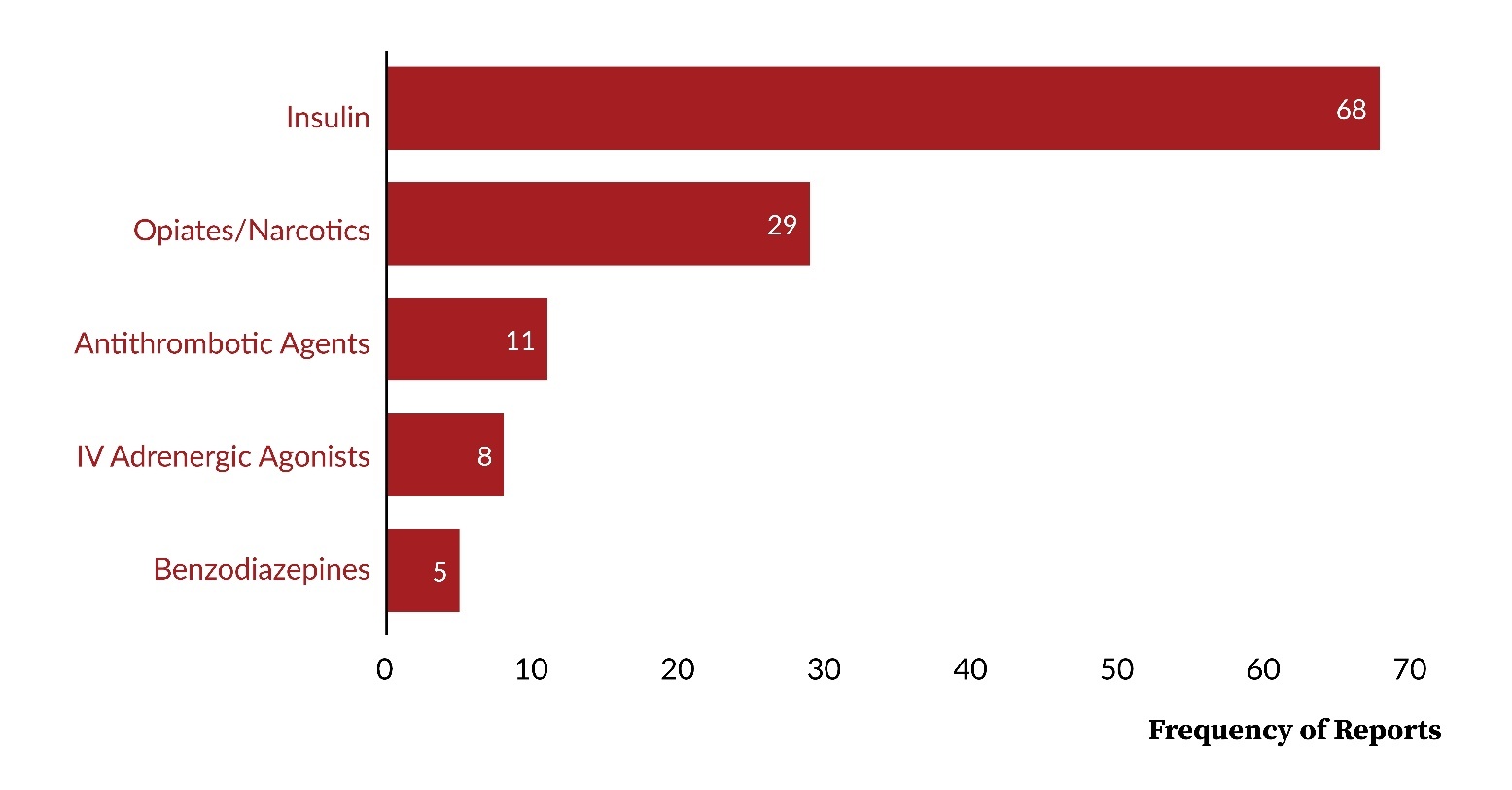
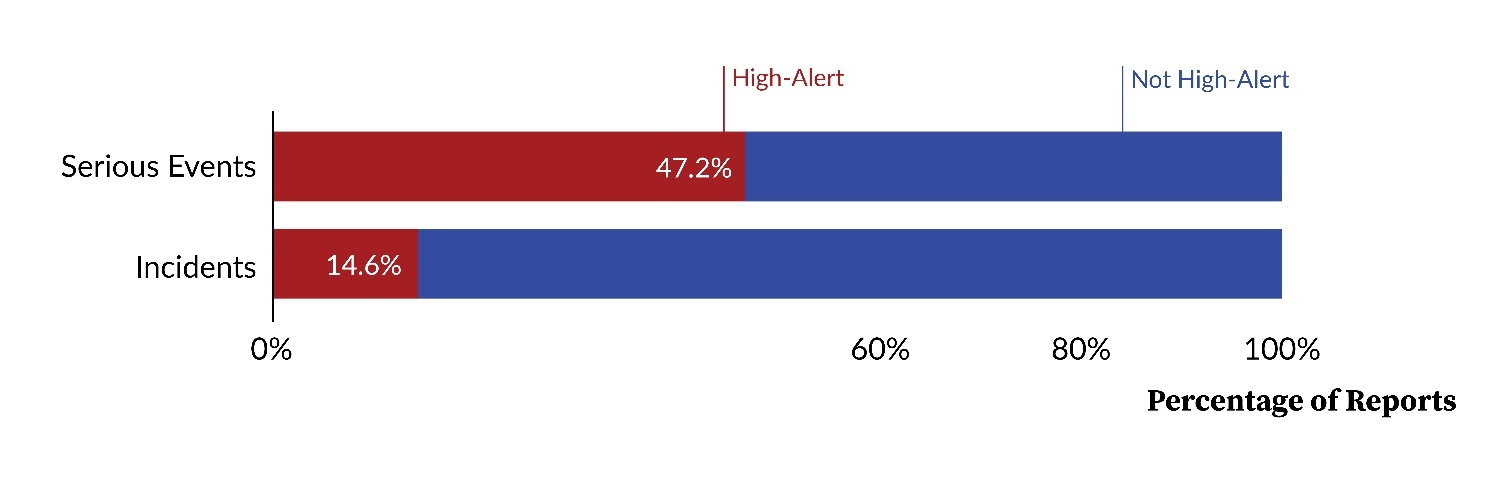
As shown in Figure 1, high-alert medications were reported to PA-PSRS in association with serious Medication Error events at a proportion more than three times higher than for incidents[2];1 in 2025. Among the serious events, insulin was the most frequently reported high-alert medication, followed by opiates/narcotics and antithrombotic agents, as displayed in Figure 2.
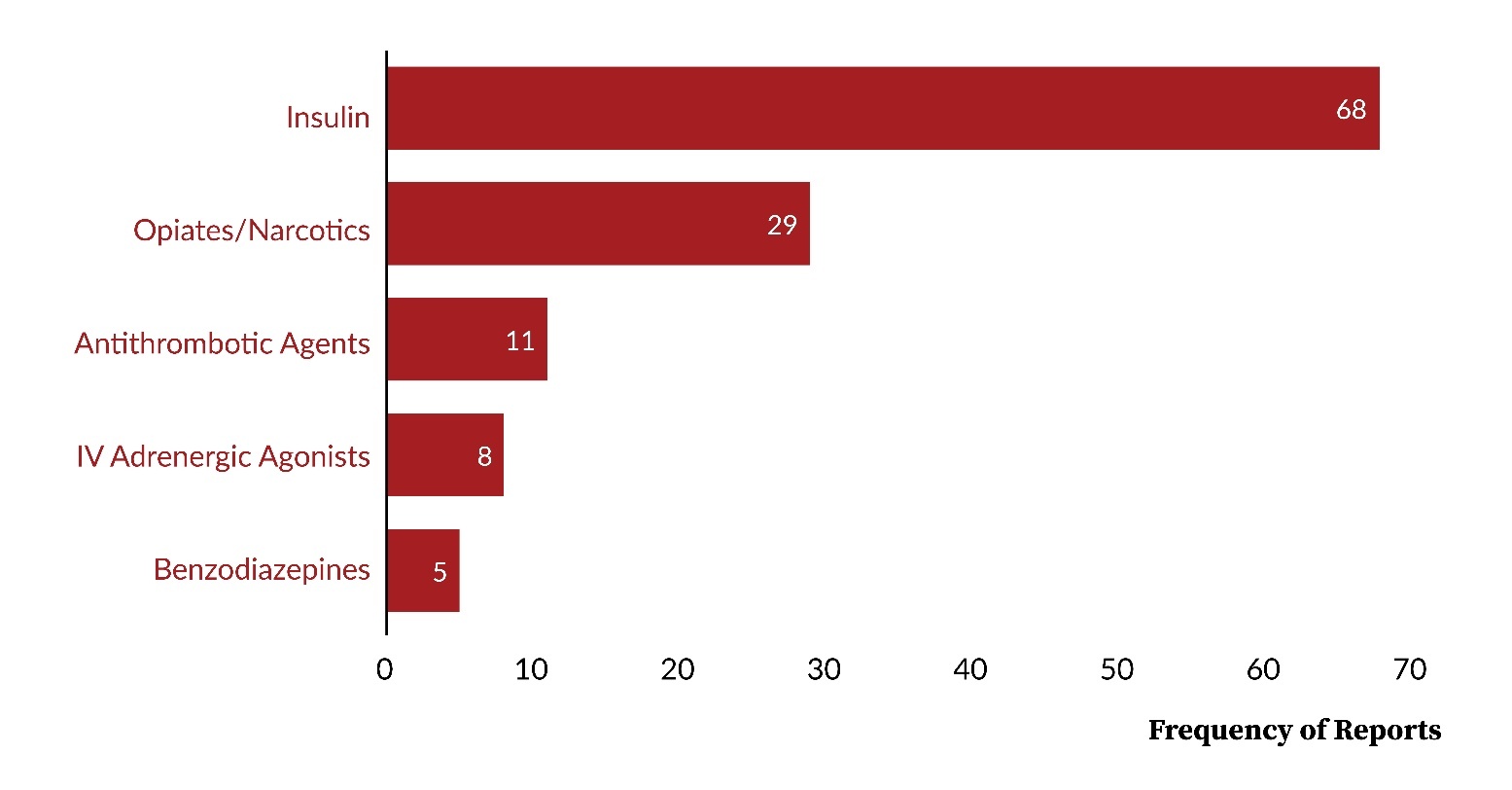
It is important to note that, although nifedipine as an individual medication is not included in the Institute for Safe Medication Practices (ISMP) List of High-Alert Medications3 and therefore not currently listed as a high-alert medication in PA-PSRS, it was involved in the same number of serious medication events as the entire class of high-alert benzodiazepines (5 reports). Previous PA-PSRS analyses have linked nifedipine-related errors to serious patient harm, including death.4
Patterns of Error and Clinical Impact
Analysis of serious Medication Error events reported to PA-PSRS in 2025 shows persistent, high-risk patterns. Insulin remains a major source of errors and inadvertent harm; PSA publications in 2025 identified insulin as the medication class most frequently involved in wrong-drug errors5 and associated it with large-scale overdoses resulting from syringe-related errors.6 Since our earlier newsletter highlighting fivefold wrong dose errors with U-500 insulin,7 the manufacturer has discontinued U-500 vials in the United States.8,9 Wrong drug errors involving other medications also continue, including a fatal event in which 0.5 milligrams epinephrine was administered instead of 0.5 mg atropine, and an event in which 99% dehydrated alcohol was accidentally injected into a patient’s eye due to the alcohol sharing a storage location with the intended medication containing a mixture of lidocaine and epinephrine. Lastly, wrong-route errors persist. In one case, preservative-containing morphine was administered intrathecally (i.e., directly into the cerebrospinal fluid) at 10 times the intended dose despite the fact that intrathecal administration of preservative-containing morphine is contraindicated.10 In another case, sucralfate intended for administration via a feeding tube was given through a central line after instructions noting “oral vs tube administration” were interpreted as intravenous “tube” administration. These recurring themes highlight the ongoing need to revisit previously published strategies to mitigate wrong-route errors.11,12
Takeaways
Although serious events comprise a small fraction of all medication error reports submitted to PA-PSRS in 2025,2 the potential for serious patient harm should not be underestimated: At least six reports were associated with death or transition to comfort care. While high-alert medications were involved in almost half of the serious Medication Error events, serious patient harm can occur with the inappropriate use of any medication. Facilities are encouraged to reevaluate their current safety practices, identify any gaps in their workflow and protocols, and implement necessary changes to reduce the risk of serious patient harm associated with medication errors.
Disclosure
The author declares that they have no relevant or material financial interests.
Artificial intelligence (Copilot Chat) was used only to improve sentence clarity. No AI was used for data analysis, interpretation, or generation of original content. The authors take full responsibility for the accuracy and integrity of the manuscript.
This article was previously distributed in a May, 5, 2026, newsletter of the Patient Safety Authority, available at https://patientsafety.pa.gov/newsletter/Pages/newsletter-may-2026.aspx.
About the Author
Myungsun (Sunny) Ro (mro@pa.gov) is a research scientist on the Data Science & Research team at the Patient Safety Authority (PSA). Her responsibilities include analyzing and synthesizing data from various sources to identify opportunities to improve patient safety, as well as writing scientific articles for publication in the PSA’s peer-reviewed journal, Patient Safety.
A serious event is defined as “an event, occurrence, or situation involving the clinical care of a patient in a medical facility that results in death or compromises patient safety and results in an unanticipated injury requiring the delivery of additional healthcare services to the patient.”
An incident is defined as “an event, occurrence, or situation involving the clinical care of a patient in a medical facility which could have injured the patient but did not either cause an unanticipated injury or require the delivery of additional healthcare services to the patient.”