







The Patient Safety Authority (PSA) established the annual I AM Patient Safety (IAPS) Achievement Awards1 to celebrate staff at Pennsylvania hospitals and facilities for their extraordinary accomplishments on behalf of patients.
IAPS is a peer-nominated contest that invites anyone to nominate an individual or a team for an award in Ambulatory Care, Commitment to Safety, Healthcare Disparity, Improving Diagnosis, Individual Impact, Medication Safety, Patient Communication, Safety Story, and Transparency. For the 2026 awards, a jury of patient safety advocates; government, university, and patient representatives; and healthcare executives evaluated 169 nominations from 72 healthcare facilities. In addition to the nine winners that they selected for their innovation, impact, sustainability, and scalability, Regina Hoffman, MBA, RN, selected the winner of the Executive Director’s Choice Award for special recognition.
Every IAPS nominee deserves thanks and congratulations for their efforts, accomplishments, and contributions to patient safety. Many of their inspiring stories will be shared through PSA’s Lessons From Event Reports microsite as examples of how event reporting has helped effect change and improve care.2
Executive Director’s Choice Award
Mollie Herlehy

A young trauma patient diagnosed with rib fractures, brachial injury, and C-spine fracture was experiencing cognitive deficits, which providers initially believed were related to a concussion. Speech pathologist Mollie Herlehy completed a comprehensive cognitive exam and advocated strongly to have further imaging for this trauma patient. Additional imaging was conducted, and the patient was noted to have had several embolic strokes and a carotid dissection requiring emergent transfer to a higher level of care. The team acted quickly, and the patient received appropriate treatment. The patient returned to see and thank the staff, including Herlehy, after their recovery.
Herlehy was patient-center focused, advocated for the patient, and demonstrated willingness to speak up for their safety and quality of care, resulting in an overall positive outcome. All staff are educated and encouraged to speak up for patient safety and use the phrase “I need clarity” when a potential or actual patient safety concern happens. Herlehy leads as an example of the positive impact this practice can have on patients.
Safety Story Award
Shantel Thomas and Daniel Blum

During a surgical procedure, the nurse, Shantel Thomas, and surgical technician, Daniel Blum, were performing their closing count when they identified that one laparotomy sponge was unaccounted for. Despite the surgeon’s assurance that the sponge could not be inside the patient due to the presence of an AbThera dressing, they remained steadfast in their concern. They respectfully but firmly reiterated that their count was off and that the missing sponge had to be located. Their persistence prompted the surgeon to remove the dressing—and the missing sponge was found.
Thanks to their vigilance, assertiveness, and unwavering advocacy for patient safety, the duo prevented a retained surgical item, which could have led to serious complications for the patient. Their actions exemplify the highest standards of intraoperative care and reinforce the importance of speaking up and trusting the surgical count process.
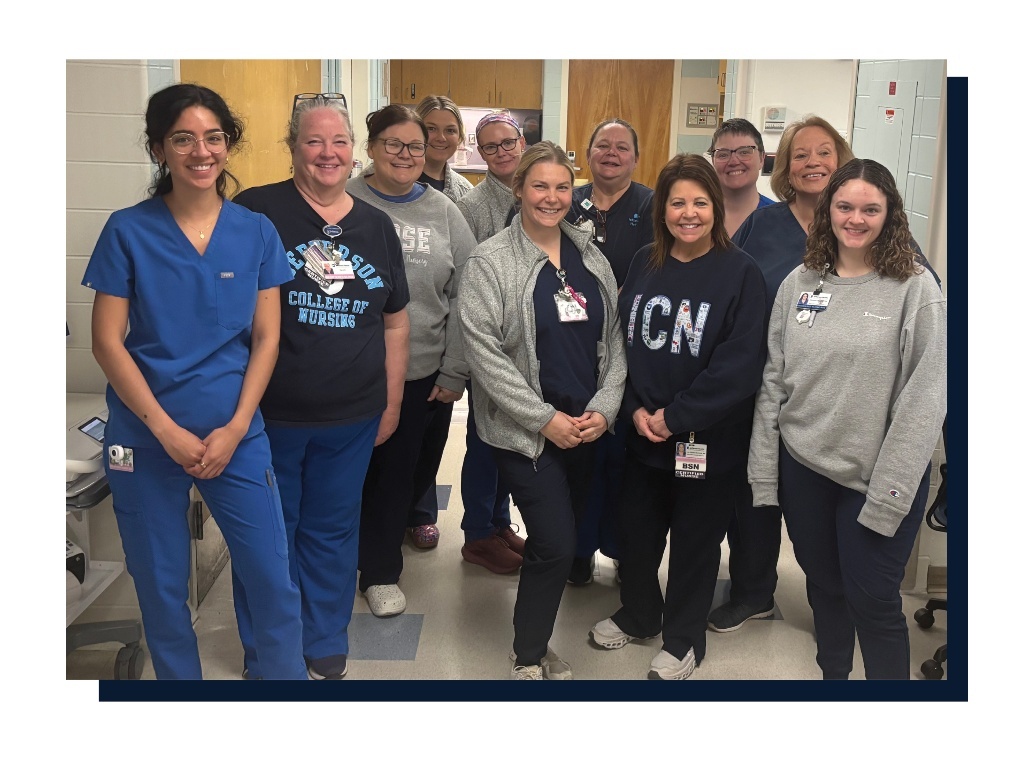
Medication Safety Award
Heather Etzl and the Intensive Care Nursery Team

Barcode scanning of medications is an effective way to reduce medication errors. The barcode scanning workflow in the Intensive Care Nursery (ICN) was frequently bypassed or manipulated to prevent having to disturb infants at the time of scanning. Some infants’ barcodes were affixed to objects at their bedside rather than on the infant, and sometimes the barcode scanning process was circumvented completely. This problem was recognized during a monthly review of incident reports in multidisciplinary Quality and Safety Committee meetings.
Surveys were distributed to the nursing staff to better understand the reasons for variability in barcode scanning practices, and a simple but elegant solution was developed to address the issue: The clinical practice leader, Heather Etzl, identified and purchased tethers that can be attached to an infant’s ankle and display the medication barcode outside of their clothes or blankets rather than directly at their skin, avoiding the need to disturb the infant to scan their barcode. Education was distributed to explain the proper use of the tethers and encourage their use by citing previous medication errors that could have been prevented by proper barcode scanning.
Etzl then conducted several months of audits to ensure the tethers were being properly used. During that time, the ICN team identified several barriers to proper placement and improved accessibility to the tethers if they needed to be replaced. Proper attachment of the barcode on infants’ extremities improved from 34% to 100% by the second month after introduction of the tethers. In the months following implementation of this process, the unit had two “good catches” where proper barcode scanning prevented medication errors. Identification and improvement of this safety concern took a multidisciplinary approach within the ICN with Heather Etzl spearheading the effort.
Improving Diagnosis Award
CAUTI Prevention Team

The organization identified an ongoing challenge with higher-than-expected catheter-associated urinary tract infection (CAUTI) rates. A multidisciplinary team has been in place for several years investigating potential causes and opportunities for improvement; as part of this work, they conduct case reviews after any identified CAUTI event. The reviews recently identified a trend towards inappropriate ordering of urine studies in response to fevers, even when an identified alternate cause of fever was evident. These clinically inappropriate urine cultures led to potential patient harm, as they prompted unnecessary antibiotic exposure, and institutional harm, because they led to events being attributed as CAUTIs when they clinically were not. In response to these findings, the team undertook a quality improvement project to reduce clinically inappropriate urine cultures and improve the diagnosis of urinary tract infections (UTIs) in the organization.
The team began by reviewing the medical literature and found that inaccurate diagnosis of UTI was not uncommon, and studies estimate that up to 73% of UTI diagnoses may not be accurate. Furthermore, studies have shown that a majority of these patients still receive inappropriate antibiotics, and they account for inaccurate attributions of CAUTI. Diagnostic stewardship increasingly is being identified as an opportunity to improve urine testing and UTI diagnosis. A large, multicenter study from Michigan found that reductions in inappropriate treatment of asymptomatic bacteriuria were driven more by diagnostic stewardship interventions over antibiotic stewardship. Therefore, the improvement team decided to devise and implement two diagnostic stewardship interventions.
First, the team created a new urinalysis (UA) with reflex urine culture workflow. Literature shows that UA has a high negative predictive value, and utilization of parameters to only perform cultures on specimens with an abnormal UA reduces inappropriate diagnosis. Next, the team reviewed the ordering practices of clinical staff and found that urine studies were commonly entered in patients without symptoms of UTIs. The positive predictive value of UA is very low, so performing an assessment for symptoms prior to ordering studies is essential. Since clinical decision support (CDS) has been shown to improve diagnosis and reduce inappropriate studies, the team developed a clinical workflow within the electronic health record (EHR) which prompts clinicians to assess and document symptoms of UTI and, if none are present, prompts the ordering clinician to cancel the urine studies.
Utilizing these two CDS tools, the improvement team achieved a 35.9% reduction in total urine culture orders, an improvement in the CAUTI standardized infection ratio, and overall improved accuracy of diagnoses of UTIs.
Commitment to Safety Award
Mobility Champion Team led by Jean Romano, Shawn Parsons, Sonya Wood-Johnson, and Lindsay Furlong

GSPP Rehabilitation’s inpatient rehabilitation facility and long-term acute care hospital (LTACH) developed an innovative plan to address three key, interrelated areas of patient care and employee safety. In January 2023, a Mobility Champion team of registered nurses (RNs), certified nursing assistants (CNAs), therapists, and therapy aides was launched to engage frontline clinicians and combine efforts collaboratively. The role of the champions is to serve as peer mentors and change agents by using advanced knowledge, skills, and strategies to improve patient outcomes and reduce harm. Each interdisciplinary member of the champion team selects one of three focus areas: pressure injury prevention, fall reduction, and safe patient handling and early mobility.
The original team consisted of 12 champions and four leaders and more than doubled in 18 months to include 30 very engaged frontline members. The increase in members is directly related to a few of the champions going above and beyond recruiting new members. The entire team meets quarterly for eight-hour retreats to receive advanced training, review and analyze data, identify root causes, and develop strategies for improvement. The three subgroups then meet monthly to guide and refine action plans, identify educational opportunities, and plan implementation of changes in practice.
Each of the subgroups has implemented targeted interventions to improve and impact patient-centered care by reducing unassisted fall rates, preventing new pressure injuries, healing existing wounds prior to discharge, and preventing employee and patient injuries by using proper transfer techniques and available repositioning and transfer equipment.
The Safe Patient Handling and Early Mobility subgroup implemented a “no boost campaign,” which reduces the risk of injury to staff while eliminating risk for shear and injury to patient’s skin. They also conducted hands-on training sessions promoting safe transfer techniques. Total employee injury claims have been reduced by 38% since the program’s inception.
Specific interventions to reduce pressure injuries include the utilization of a repositioning monitor system to ensure frequency and proper off-loading; implementation of several best practice trainings, including “less is best”; and education on the appropriate ointments and prophylactic foam dressings. The percentage of unhealed pressure injuries declined from 7% pre–champion implementation to 0.7%.
The team focusing on reduction of unassisted falls provided hands-on training; creation of huddles; implementation of post-fall team huddles to identify opportunities for improvement; ceiling tiles to remind patients to “call, don’t fall”; signage in the rooms and bathrooms to maintain direct visualization; and implementation of personal caddies for patients to store phones, chargers, etc. to prevent reaching. Unassisted falls have declined by 31% overall, with significant reductions in bathroom falls and reaching-related falls.
The sustainability of this work is unequivocally correlated to the commitment and engagement of the frontline nursing and therapy team members. This team recently shared their efforts and the results with other members of the rehabilitation community at a recent American Medical Rehabilitation Providers Association conference, allowing for the spread of the concept to other organizations. The podium presentation generated strong interest and positive feedback.
Patient Communication Award
Respectful Care Breakfast Team
Respectful maternity care is essential to ensuring safe, equitable, and high-quality obstetric outcomes. Yet, a persistent gap remains between the care patients receive and their personal experience of that care. In response to this challenge, a multidisciplinary team at Penn Medicine developed and implemented the Respectful Care Breakfasts (RCBs), bimonthly sessions where postpartum patients can share their birth experiences directly with a diverse group of care providers, including nurses, physicians, midwives, social workers, nurse managers, and hospital leadership. Staff participate exclusively as listeners, setting aside hierarchy and clinical roles to simply hear and honor patient voices.
The simple format of breakfast conversations grounded in open-ended questions represents a creative, effective, and low-cost solution to a pervasive challenge: the disconnect between clinical care and patient experience. Rather than relying on traditional metrics or surveys, the team created a unique forum that illuminates blind spots in care delivery while fostering connection across roles and disciplines.
The initiative has had an impact on both care quality and team culture. Post-event patient surveys showed high satisfaction (mean rating: 4.8/5), with participants expressing profound appreciation for being heard in a nonclinical setting. Healthcare staff reported a renewed commitment to respectful maternity care and greater insight into patient needs. Importantly, the RCBs catalyzed changes in practice, such as signage for birthing parents separated from their newborns—a patient-identified gap that was promptly addressed.
Over a 12-month period, the RCBs have become an embedded and valued part of the hospital’s maternity care strategy, centering patients as active partners in shaping safer, more respectful systems.
Healthcare Disparity Award
Lebanon County Crisis Intervention and Referral Services

Crisis intervention is a mandated service in every Pennsylvania county and has been in place for decades. Lebanon County’s program had long served as a vital access point for individuals in behavioral health crisis, but their team observed that many individuals accessed their services through the emergency department (ED) before being referred for outpatient follow-up. In response, they sought to expand their community presence through mobile and walk-in services. This approach allows the team to “meet people where they’re at,” in alignment with national guidelines for behavioral health crisis care.
Lebanon County Crisis Intervention and Referral Services is a vital, county-funded program dedicated to serving all individuals throughout the community. This service is provided completely free of charge, ensuring that no one is turned away due to insurance status. Whether someone is uninsured, underinsured, or fully covered, this program offers compassionate, professional support to anyone in need 24/7. The program reflects the county’s commitment to accessible mental health and crisis services for every resident, regardless of background or financial situation.
This program has made transformative progress in advancing patient safety through community-based mental healthcare. Over fiscal year 2025, the team worked tirelessly to shift the paradigm from reactive emergency responses to proactive, compassionate engagement in the community. They saw a 68% increase in mobile crisis responses and a 44% increase in walk-in visits compared to FY 2024. These numbers reflect a deliberate and strategic effort to expand access to care outside of hospital settings. By embedding themselves more deeply in the community, they have been able to intervene earlier, de-escalate crises more effectively, and guide individuals toward appropriate services—often avoiding the need for ED visits or inpatient hospitalization.
While ED visits slightly rose by 2.6% in FY 2025 compared to FY 2024, a broader analysis of the previous three years (2020–2023) shows a 10% overall decrease in ED utilization, signaling a meaningful long-term trend. Most notably, the program achieved a 9% reduction in involuntary commitments in FY 2025, despite the total number of patients requiring hospitalization remaining consistent. This shift is a powerful indicator of improved patient engagement and trust. When patients understand and agree with care recommendations, they are more likely to participate voluntarily, resulting in safer, more respectful treatment experiences.
The program’s approach centers on collaborative care. When a patient is in crisis, the team not only assesses their needs but also walks alongside them through the next steps—whether that means connecting them with outpatient services, coordinating with family supports, or facilitating voluntary inpatient treatment. This model fosters dignity, autonomy, and empowerment, which are essential components of patient safety in behavioral health.
The team believes that patient safety is not just about preventing harm—it’s about creating systems of care that are responsive, humane, and equitable. Their success is a testament to the power of community engagement, early intervention, and trauma-informed care. By reducing involuntary hospitalizations and increasing voluntary participation, they are helping patients feel seen, heard, and supported.
Ambulatory Care Award
St. Margaret Dermatology Clinic

The St. Margaret Dermatology Clinic staff has made an innovative contribution to advancing surgical safety in their high-volume ambulatory surgical center. As the clinic is hospital-based, its staff became more engaged with the UPMC St. Margaret safety team, including in biweekly safety event reviews. In one of these meetings, the clinic staff identified that they had safety events that were not being reported. Risk education was provided to the clinic to increase capture of events, near misses, and good catches. With their increased awareness of event reporting, clinic staff set a goal to eliminate wrong-site surgeries (WSS) in the Dermatology Clinic through standardized verification and team engagement.
Specializing in the removal of skin cancers and other lesions through excision and Mohs surgery, the clinic operates six surgical suites and performs 10–20 cases daily in a fast-paced environment, often requiring a quick turnover of procedure rooms with patients quickly moving in and out of the procedure rooms. Recognizing an increase in WSS—a serious “never event”—the team acted promptly and collaboratively to design and implement a process to eliminate these occurrences and enhance patient involvement in safety.
After a productive root cause analysis (RCA) with the Quality and Dermatology teams, they developed and implemented a comprehensive action plan that included:
Enhanced Time-Out Protocol
A time-out is now conducted before each staging procedure during Mohs surgery, even if multiple stages occur in the same session. Visual reminders were introduced, including plaques placed on counters and designated time-out sections on Mohs maps.
Real-Time Communication
Headsets were purchased for all surgical staff, ensuring immediate communication and confirmation that all required team members are present during critical safety checks.
Patient Engagement
Larger handheld mirrors were provided so patients can visually verify the surgical site alongside the provider, reinforcing transparency and shared responsibility for safety.
This innovative approach has significantly reduced the risk of WSS, strengthened team communication, and empowered patients to actively participate in their care. The process improvements have created a safer surgical environment and set a new standard for patient-centered safety practices in ambulatory dermatology care. The Dermatology ambulatory surgical team exemplifies the principles of patient safety through proactive problem-solving, collaboration, and innovation. Their commitment to preventing harm and engaging patients sets a benchmark for excellence in ambulatory surgical care.
Individual Impact Award
Amanda Yingst

During a routine preoperative phone call, call room nurse Amanda Yingst demonstrated extraordinary vigilance, compassion, and commitment to patient safety. While providing standard preop instructions, she overheard escalating hostility from the patient’s significant other. Recognizing the signs of potential domestic violence, she immediately shifted her focus to assessing the patient’s safety. With exceptional sensitivity, Yingst asked direct yet supportive questions regarding the situation at home. The patient disclosed that she did not feel safe and that her significant other was threatening to take away access to her phone because of the information being shared with Yingst. The patient added that her surgery was necessary due to ongoing physical abuse at home, further exacerbating her medical condition.
Understanding the urgency of the situation, Yingst calmly assured the patient that she would call back shortly with updated information and ended the call to prevent further escalation. This provided the opportunity for the patient to state it was necessary for her to continue using the phone. Yingst promptly notified the surgeon, Dr. Michael McDowell, relaying her concerns and emphasizing the immediate risk to the patient. After obtaining the necessary information, Dr. McDowell contacted local law enforcement and requested a welfare check, as well as EMS transport to ensure the patient could be brought to a safe environment for the night and subsequently receive the surgery she needed the following day.
Because of Yingst’s attentiveness, clinical judgment, and unwavering advocacy, the patient was safely removed from a threatening environment. Yingst’s ability to recognize subtle cues, act swiftly, and collaborate across disciplines exemplifies the very essence of patient-centered care. This situation highlights not only her outstanding clinical skills, but also her courage and dedication to protecting patients beyond the walls of the hospital. Her actions went far beyond the expectations of her role and directly contributed to preventing potential harm, ensuring that one patient—on one vulnerable day—was heard, protected, and kept safe.
Transparency Award
Jefferson Abington and Lansdale Hospital Patient Safety & Quality Team

The Great Catch–Great Save Program at Jefferson Abington and Lansdale Hospital recognizes employees who go above and beyond to protect patients and improve hospital systems. This initiative highlights individuals who intervene before harm occurs, identifies near-misses, and uncovers opportunities for system redesign. These actions are celebrated weekly, monthly, and quarterly across various venues—from peer-level recognition to acknowledgment by senior leadership.
To further promote transparency and learning, the Patient Safety & Quality Team developed and launched a Great Catch–Great Save repository. This vetted, intranet-based platform allows all hospital employees to view and share stories of near-miss events and the resulting facilitywide improvements. Each entry not only honors the staff member’s extraordinary actions, but also details the “Safety Strategies and Behaviors” they employed—such as speaking up for safety, attention to detail, questioning and confirming, and adherence to high-reliability principles—that directly contributed to the successful outcome. Showcasing these behaviors reinforces the health system’s culture of safety and empowers others to adopt similar proactive approaches.
This transparent innovation has inspired more frontline staff to speak up and take action knowing that their contributions are valued and impactful. The Great Catch–Great Save Program has been a cornerstone of safety culture at the hospital for approximately four years and has recently expanded across Jefferson Health. After a successful pilot, the repository model has now been scaled systemwide, enabling all 32 hospitals within the health system to utilize this powerful tool for learning, recognition, and continuous improvement.
Runners–Up
Ambulatory Care
Colleen Berkery, Jefferson Surgical Center
MASC Team, Monroeville Ambulatory Surgical Center
Commitment to Safety
Surgical Services Department and Leadership (Operating Room), Milton S. Hershey Medical Center
Interdisciplinary Pressure Injury Reduction Team, WellSpan Good Samaritan Hospital
Healthcare Disparity
Sara Cohen/Women’s Health PAH, University of Pennsylvania Health System
Adult Capillary Sampling Workgroup, Pennsylvania Hospital
Improving Diagnosis
Trauma Physical Therapy/Occupational Therapy Therapists, 5N Nursing Leadership, and Gerontology, Allegheny Health Network
Andi Lint, Dr. Michael Desiderio, Lisa Sunyecz, Dr. Christine Flinn, Jessica Spiker, Stacy Pocius, Bill Johnson, Katie Tringhese, Janean Lubich, Andréa Atkinson, Heather Thompson, Dr. Ziad Dimachkie, Michelle Howard-Diggs, and Blair Lavake, WVU Medicine Uniontown Hospital
Individual Impact
Dr. Jeaninne Einfalt, Lehigh Valley Hospital-Cedar Crest
Emily Rzodkiewicz, UPMC Hamot
Medication Safety
Neil Wetcher, Lehigh Valley Hospital-Muhlenberg
Diana Colonna and the Pediatric Intensive Care Unit Team, St. Christopher’s Hospital for Children
Patient Communication
Medicine and Behavioral Health Clinical Effectiveness teams, Hospital of University of Pennsylvania
Lindsey Morris and Jimmy Landy, UPMC Hamot
Safety Story
The Philadelphia Campus Behavioral Health Clinician Team, Children’s Hospital of Philadelphia
Dr. Vivek Ahya, Dr. Julie Uspal, and Patricia Macolino, Clinical Practices of the University of Pennsylvania
Transparency
Kenneth Miller, Kimberly Smith, Robert Leshko, Salvatore Maida, and Mark Lengvarsky, Lehigh Valley Health Network-Cedar Crest
Oncology Medical Intensive Care Unit Team, Hospital of the University of Pennsylvania
Thank you to this year’s judges
Mike Bruno, MD, Penn State Health
Sophie Campbell, MSN, RN, Pennsylvania Association Directors of Nursing Administration/Long Term Care Nurses
Eric D. Dobkin, MD, Retired
Diane Frndak, PhD, MBA, Robert Morris University
Samuel Hammerman, MD, MMM, Select Medical
Regina Hoffman, MBA, RN, Patient Safety Authority
Stephen Lawless, MD, Nemours Children’s Health
Dwight McKay, Patient representative
Heidi McMullan, MSN, RN-BC, WellSpan Philhaven
Adam Novak, MS, Michigan Health & Hospital Association
Indu Poornima, MD, MS, Allegheny Health Network
Julia Prentice, PhD, Betsy Lehman Center
Marty Raniowski, MPP, Pennsylvania Medical Society
Rob Shipp, PhD, RN, The Hospital and Healthsystem Association of Pennsylvania
Eric Weitz, Esq., The Weitz Firm
Disclosure
The author declares that they have no relevant or material financial interests.
About the Author
Eugene Myers (eugemyers@pa.gov) is the associate editor of Engagement & Publications for the Patient Safety Authority. He previously served as editor-in-chief of Communications, Office of Institutional Advancement, at Thomas Jefferson University and Jefferson Health. He earned his bachelor’s degree from Columbia University, is a graduate of the Clarion West Writers Workshop, and is a New York Times bestselling and award-winning author of books for children and young adults.