Introduction
The human factors literature defines an alarm as a signal intended to capture and direct human attention to a potential issue that may require monitoring, assessment, or intervention.1 The Food and Drug Administration (FDA) and other standards organizations distinguish between alarms and alerts for medical devices by stating that alarms should be used when the operator’s awareness or response is required for risk control, while alerts provide contextual awareness that is not related to risk control.2–5 In high-risk industries like healthcare, automotive, aviation, and nuclear, alarms play a central role in identifying system malfunctions, abnormal conditions, and process deviations.2,6,7 In healthcare, alarms commonly take the form of auditory and/or visual signals embedded in medical devices and play a critical role in overall healthcare system safety and quality of care. When alarms are not designed and implemented optimally, patient harm, clinician burden, and patient frustration can occur.
Many medical devices utilize alarming to convey important information to clinicians, patients, or other users. Medical device alarms are essential to patient care and draw attention to potentially critical changes in patients’ physiological states, device malfunctions, or system status. For example, a telemetry monitor alarms staff to a dangerous cardiac arrhythmia and a dialysis machine alarms staff to serious device failures, such as impeded blood flow. While these alarms are helpful in many instances and promote patient safety, poorly designed and implemented alarms can pose patient safety risks by distracting providers from other important information.
From 2005–2010, the FDA’s Manufacturer and User Facility Device Experience (MAUDE) database received 566 reports of alarm-related patient deaths.8 Similarly, from January 2009 to June 2012, The Joint Commission’s Sentinel Event Database received 98 reports of alarm-related events, 80 of which resulted in patient deaths.8 Numerous challenges are associated with alarms that contribute to patient safety risks, including alarms not capturing the user’s attention, alarms being detected but not providing the necessary information to address the issue, and frequent inaccurate alarms (e.g., false alarms) leading users to distrust the alarms and discount them over time.9,10 The need to isolate patients during the COVID-19 pandemic has also presented increased challenges with alarm response, as patient isolation decreases staff’s ability to detect alarms.11
Alarm fatigue is the widely adopted term that describes healthcare worker desensitization to the numerous alarms in their work environments caused by high exposure to alarms.10,12 Alarm fatigue contributes to missed, delayed, or inadequate responses to alarms and may put patients at risk for experiencing adverse events.13–17 One of the many contributing factors to alarm fatigue is the number of alarms in the healthcare environment. A study analyzing physiologic monitor alarms in intensive care units found that 2,558,760 unique alarms occurred over 31 days.18 Studies have also found that many alarms, 80% to 99% by some estimates, are nonactionable or false alarms, or convey redundant information.13,16–20 Some studies have attributed the high number of false alarms in healthcare to devices’ inappropriate alarm settings and unstandardized alarm sounds.14,17,20,21
The science of human factors, which aims to understand human capabilities for the purpose of designing work environments that meet these capabilities and enable optimal human performance, has an extensive body of research to inform alarm design.22 From a human factors perspective, for an alarm to capture attention and provide appropriate information, the alarm should be detectable (i.e., heard or seen by the user), discriminable (i.e., recognized as separate from noise in the environment), and identifiable (i.e., convey the source or content of the alarm).23–28
Numerous studies in the human factors literature have systematically examined alarm features that impact detectability, discriminability, and identifiability from an auditory and visual perception perspective. For example, considering detection, movement in the visual periphery catches attention quickly, so dynamic visual alarms that change (e.g., flashing lights) are easier to detect than static visual alarms.29–31 Considering discrimination, it is easier to discriminate auditory alarms when they are distinct from the environment, specifically when the alarms are 15 decibels or louder and at a substantially different frequency than environmental noise.32,33 Considering identification, multiple studies have demonstrated that humans identify red alarms as the most hazardous, followed by orange and yellow.34–39
Several high-risk industries have applied the body of human factors knowledge about alarms to develop guidelines that inform safe and effective design and use. These guidelines often provide detailed specifications that should be adhered to in the context of the work performed. Many high-risk industries have federal agencies or other oversight organizations that have reviewed industry-specific and human factors–based guidelines and endorsed these guidelines for use. In healthcare, depending on the type of device, the FDA has some alarm-related guidelines that device manufactures should adhere to. However, some manufacturers may not follow these guidelines; many devices can be customized and configured by healthcare facilities, which may change features of the device alarms that were implemented by the manufacturer; and healthcare facilities often need to manage multiple devices that alarm. As a result, challenges with alarms in healthcare are pervasive and there is an opportunity for cross-industry learning.40–43
In this study, we sought to identify alarm design and use guidelines from high-risk industries outside of healthcare to inform healthcare practices. These guidelines may provide insights that can be adopted in healthcare environments to address the numerous alarm issues that impact patient safety. Human factors and clinical experts reviewed guidelines from the automotive, aviation, and nuclear industries to identify those most relevant to healthcare. Based on these guidelines, we provide considerations for alarming in healthcare environments.
Methods
Through an internet search, documents detailing human factors guidelines for alarm design and use endorsed by United States–based oversight agencies (e.g., Federal Aviation Administration for the aviation industry) were identified for the automotive, aviation, and nuclear industries. Two human factors experts evaluated the documents for inclusion based on the following four criteria: the publication must be endorsed by a federal government agency or be recognized by a federal government agency as applying to the industry for which the agency has oversight; be related to the automotive, aviation, or nuclear industry; contain principles, guidelines, and/or standards related to auditory and/or visual alarms; and have been published after January 2012. Each reviewer independently evaluated each document to assess whether the document met inclusion criteria, and then each document was jointly discussed to ensure agreement. Through this process, we identified one comprehensive document from each industry to be used for analysis in this study.44–46
A human factors expert extracted the title, date, agency, and specific discrete guidelines from each of the three industry documents that were included in the review and populated a Microsoft Excel spreadsheet. Guidelines were included if they contained information about visual or auditory alarms, regardless of whether they were directly applicable to healthcare, unless the guideline applied to a specific technology that was unique to that industry. For example, a guideline about using visual alarms to convey complex information would be included, but a guideline specifically about lane deviation alarms would not be included since lane deviation is specific to ground transportation. Following extraction, two human factors experts and one clinical expert reviewed each guideline to assess whether it was relevant to either inpatient or outpatient healthcare settings. A guideline was deemed relevant if it could inform the design and use of alarms in healthcare environments, regardless of whether the guideline is already being followed in healthcare. Disagreements between experts were discussed until consensus was reached. Those guidelines that were relevant to healthcare were included in the full analysis.
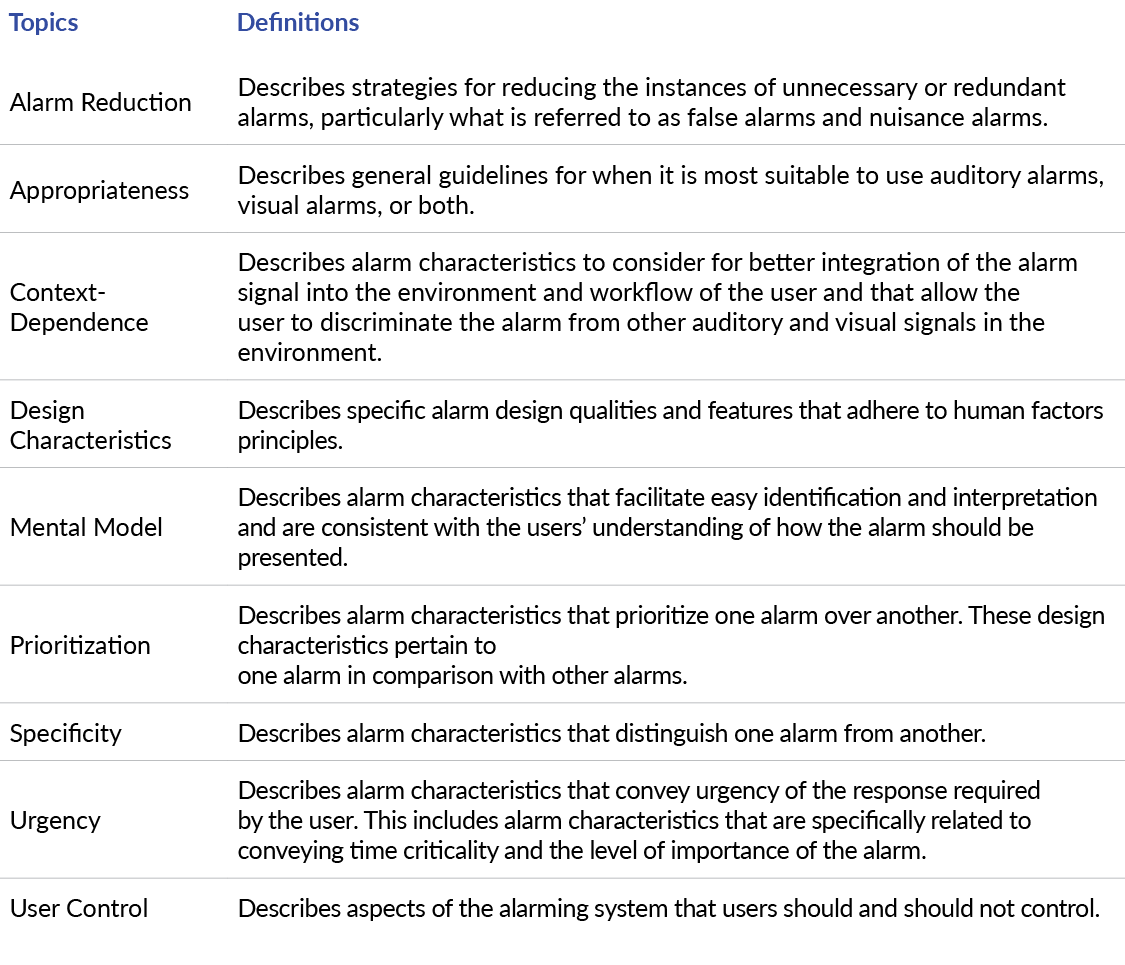
The healthcare-relevant guidelines were reviewed and grouped into meaningful topics that represented the general focus for informing alarm design and/or use. These topics were identified using a modified reflexive thematic analysis.47 Two human factors experts familiar with the data independently reviewed a subset of the relevant guidelines and assigned a label to each one to represent the overall theme. Labels were discussed and collated to create an initial set of common themes that applied to the guidelines reviewed from all three industries. Using these inductively generated topics, the human factors experts independently classified the remaining guidelines, modifying topics as necessary and discussing discrepancies until consensus was reached. Topics were reviewed for internal consistency and refined as necessary. The final topics and definitions can be found in Table 1.

Table 1.Alarm Guideline Topics and Definitions.
After classifying the relevant guidelines by topic, the guidelines were reviewed and segmented by those that applied to the auditory or visual modality, or both. The guidelines were then analyzed to identify important commonalities and differences across industries. From the general set of relevant guidelines under each topic, two clinical experts identified the two to three guidelines that were deemed to be the most highly relevant and applicable to medical devices and should be considered when designing, implementing, and managing alarms.
Results
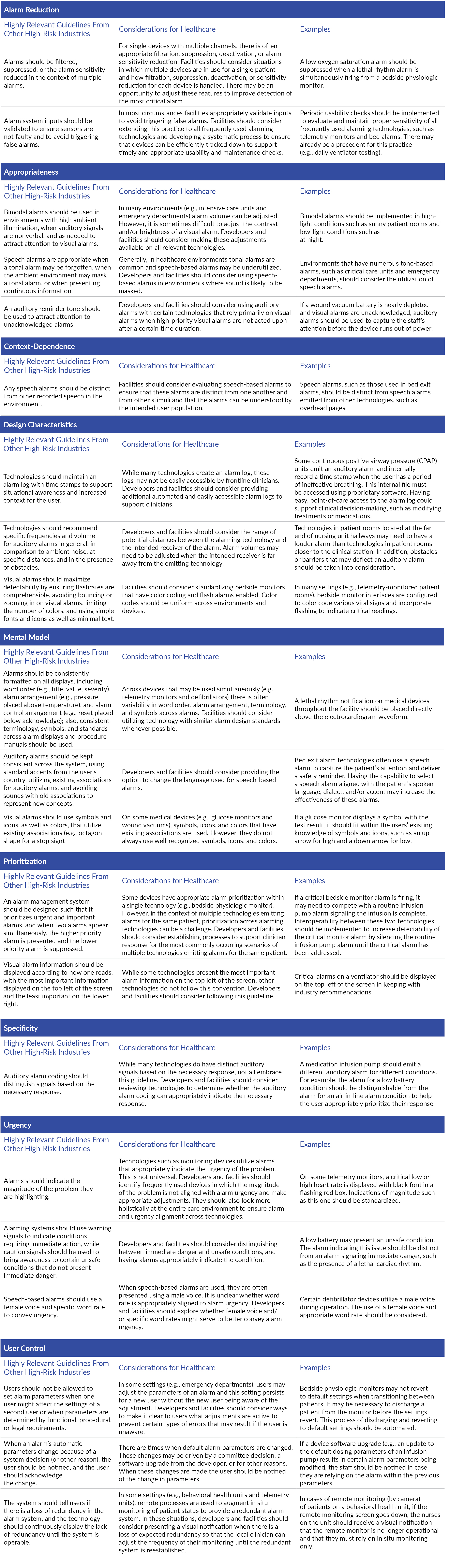
A total of 356 guidelines were extracted from the industry documents and 327 (91.9%) were deemed relevant to healthcare. By industry, 69 of 94 (73.4%) automotive industry guidelines were relevant, 148 of 152 (97.4%) aviation industry guidelines were relevant, and 110 of 110 (100%) nuclear industry guidelines were relevant. A comprehensive list of all the relevant guidelines can be found in Online Supplement Appendix A. In Online Supplement Appendix B, we provide a summary of commonalities and differences, organized by topic and segmented by applicability to visual and auditory modalities, auditory only, and visual only. Table 2 describes the most highly relevant guidelines applicable to medical devices that were identified as potentially having implications for healthcare settings along with considerations for technology developers (“developers”) and healthcare facilities (“facilities”), with examples for each.

Table 2.Summary of the Guidelines Highly Relevant and Applicable to Medical Device Design From Other High-Risk Industries, Considerations for Healthcare, and Examples per Alarm Guideline Topic.
Note: Some of the practices identified in these examples may already be in place in some healthcare facilities.
Discussion
Our analysis of guidelines from the automotive, aviation, and nuclear industries identified numerous guidelines to inform alarm design and use. Unsurprisingly, there were often similarities across the industries, which was expected considering these guidelines were informed by the same body of human factors literature and theories of auditory and visual perception. Given variations in work environments, there were also differences across the industry guidelines, as they need to be relevant to the specific work conditions and tasks for each respective industry. These findings provide insights that may be relevant to healthcare and can inform alarm design and use for multiple stakeholders, including medical device manufacturers, healthcare facilities, and healthcare oversight organizations.
While many of the guidelines reviewed from other high-risk industries have implications for healthcare and we have described how healthcare stakeholders might consider applying these guidelines (Table 2), there are significant differences between healthcare and other high-risk industries that should be noted. Most high-risk industries have greater control over the specific technologies that are used in their industry as compared to healthcare, which makes it easier to standardize alarm features. Further, having greater control over technologies enables alarm management systems, which are software tools that can support coordination and prioritization of alarms. The FDA provides some guidance on alarm management principles and regulatory requirements, and standards exist; however, software systems that manage alarms are not as prevalent as in other industries. A critical next step for healthcare is to implement alarm management software systems that can coordinate alarms across medical devices, as well as other technologies. Other high-risk industries typically have a limited number of human users in the control room or operating area of the work environment, which enables greater customization to the needs of those users. Another difference is that in healthcare the condition of the patient can be highly variable, whereas in other high-risk industries like aviation and automotive, the condition of the airplane or vehicle is more constant. The variability of patient condition adds tremendous complexity to alarm design and use.
In the absence of tighter controls and higher levels of standardization in healthcare, it will be difficult to apply all the guidelines and principles outlined in this report. However, these high-risk industry guidelines can serve as a framework for discussions with medical device manufacturers to optimize safe and usable alarm parameters, evaluate new products being considered for procurement, and to evaluate and optimize the alarms in the current work environment. These guidelines can also provide a basis for developing internal policies and standards surrounding alarm parameters within a hospital or healthcare system. In essence, these guidelines provide a different lens on the alarm challenges that plague healthcare and may inspire new ideas for effective alarm design and use in the future.
One significant difference between healthcare and the other high-risk industries we analyzed is the level of autonomy at each healthcare facility compared to the work environments in other industries. In aviation, the cockpits across airplanes that are the same model are generally standardized regardless of what airline company is operating the airplane. In the nuclear industry, the control rooms are generally standardized, and the technology being implemented is tightly controlled. In the automotive industry, the in-vehicle technologies are also tightly controlled and there is standardization across the same models of vehicles. While there is a high degree of standardization and regulation, these high-risk industries also have a higher degree of control over the design of their in-house alarm systems. In healthcare, the care environments are often not standardized and several different technologies from different manufacturers or developers may be implemented, customized, and configured at a facility level. Consequently, if general guidelines are followed by a manufacturer or developer, when this technology is used in the actual care environment, it may be used with other technologies that were not considered by the manufacturer or developer. Further, the technology may be customized or configured by a healthcare facility, resulting in deviations from the guidelines.
Policies and Guideline Adoption
The automotive, aviation, and nuclear industries each have at least one federal agency that is, at a minimum, endorsing guidelines to inform the design and use of alarms. These guidelines provide important knowledge to promote greater safety in these high-risk industries. In healthcare, there are few guidelines endorsed by federal agencies to promote safety in a similar fashion to other high-risk industries. The FDA provides some guidelines for medical device manufacturers, as do certain standards organizations, and certain devices require usability testing; however, this is not true for all devices.2–5 Further, manufacturers are not required to test the device in the context of other devices that also alarm. Organizations such as the Agency for Health Research and Quality, The Joint Commission, and the Association for the Advancement of Medical Instrumentation offer guidelines that address issues of alarm fatigue and summarize best practices surrounding alarm management and risk reduction.43,48,49 However, these guidelines may not be easily accessible and widely used by frontline decision-makers and biomedical engineers in the healthcare facilities adopting alarming medical devices. There is an opportunity for federal and state agencies overseeing healthcare safety to provide more specific guidelines for medical device manufacturers and to identify ways to promote guideline adoption by the healthcare facilities using these devices.
To address this issue, organizations like The Joint Commission or the Centers for Medicare and Medicaid Services could provide basic guidelines for healthcare facilities to adhere to around alarming. This would address the issue of differences between healthcare facilities and the customization and configuration of alarms. These organizations could establish basic safety guidelines to influence the number of alarming devices and characteristics of the alarms.
Limitations and Future Work
There are limitations to our study. The alarm guidelines were based on an internet search, and we sought to retrieve the latest version of the guidelines that were publicly available. However, other guideline documents may exist or more recent versions of the guidelines we reviewed may exist in a private domain. The determination of relevance of the guidelines to healthcare is based on a qualitative assessment and some guidelines deemed to be relevant may not be relevant in a particular context. Similarly, guidelines that were deemed to be irrelevant may be relevant in certain contexts.
There are important opportunities to expand this work. First, these guidelines that have been sourced from other high-risk industries should be compared with guidelines, standards, and regulations from the FDA and other healthcare stakeholders to identify which cross-industry guidelines are unique. Second, the guidelines should be evaluated to determine their effectiveness at addressing alarm safety issues in healthcare.
Conclusions
Effective alarm design and use in healthcare is imperative for patient safety. Human factors–informed alarm guidelines from other high-risk industries provide insights for safe alarm use in healthcare. A review of alarm guidelines from the automotive, aviation, and nuclear industries identified key topics and specific guidelines that should be considered by healthcare stakeholders to improve alarm use in healthcare. These guidelines can serve as a framework for medical device manufacturers and healthcare facilities to evaluate current alarm design and use. In addition, there are opportunities for improved policies from oversight agencies to address alarm safety.
About the Authors
Zoe M. Pruitt is a senior human factors specialist at the MedStar Health National Center for Human Factors in Healthcare.
Lucy S. Bocknek is a human factors and safety scientist at the MedStar Health National Center for Human Factors in Healthcare.
Deanna-Nicole C. Busog is a senior research associate at the MedStar Health National Center for Human Factors in Healthcare.
Patricia A. Spaar is a senior clinical safety and research specialist at the MedStar Health National Center for Human Factors in Healthcare.
Arianna P. Milicia is a research associate at the MedStar Health National Center for Human Factors in Healthcare.
Jessica L. Howe is a research scientist and system safety specialist at the MedStar Health National Center for Human Factors in Healthcare.
Ella S. Franklin is the senior director of nursing research and systems safety science at the MedStar Health National Center for Human Factors in Healthcare.
Seth Krevat is the senior medical director at the MedStar Health National Center for Human Factors in Healthcare and an assistant professor at Georgetown University School of Medicine.
Rebecca Jones (rebejones@pa.gov) is director of Data Science and Research at the Patient Safety Authority and founder and director of the PSA’s Center of Excellence for Improving Diagnosis.
Raj M. Ratwani is the director of the MedStar Health National Center for Human Factors in Healthcare, vice president of scientific affairs at the MedStar Health Research Institute, and an associate professor at Georgetown University School of Medicine.
Disclosure
The authors declare that they have no relevant or material financial interests.
Article available at doi.org/10.33940/med/2023.3.1
Patient Safety Vol. 5, No. 1 (March 2023)
This supplementary material has been provided by the authors to give readers additional information about their work.
How to Cite the Original Article
Pruitt, Z.M., Boxknek, L.S., Busog, D.C., Spaar, P.A., Milicia, A.P., Howe, J.L., . . . Ratwani, R.M. Informing Healthcare Alarm Design and Use: A Human Factors Cross-Industry Perspective. Patient Safety, 5(1), 6–14. https://doi.org/10.33940/med/2023.3.1
How to Cite This Online Supplement
Pruitt, Z.M., Boxknek, L.S., Busog, D.C., Spaar, P.A., Milicia, A.P., Howe, J.L., . . . Ratwani, R.M. Online Supplement to “Informing Healthcare Alarm Design and Use: A Human Factors Cross-Industry Perspective.” Patient Safety, 5(1), i–xviii. https://doi.org/10.33940/med/2023.3.7
Appendix A. Guidelines (Exact Text) From the Automotive, Aviation, and Nuclear Industries Related to Alarming/Alerting
In Appendix A, we provide a comprehensive list of relevant guidelines from other industries. We have used language aligned with what is stated in the source documents. Many industries use the term “alert” in addition to “alarm” without differentiating between the two terms. Thus, the term “alert” appears below.
To access Appendix A, please download the Online Supplement using the Data Sets/Files link at the top of this page.
Alarm Reduction
Guidelines Applicable to Visual and Auditory Modalities. All three industries recommend filtering, suppressing, and reducing detection sensitivity to minimize false or nuisance alarms and reduce annoyance, engender trust in the system, and bolster alarm effectiveness. The nuclear and aviation industries recommend that alarm system inputs be validated to ensure that sensors are not faulty to avoid triggering false alarms. The nuclear and aviation industries also recommend that if a single event leads to subsequent related alarms, only the alarm that triggered the event should be presented.
The automotive industry recommends that alarm systems use redundant inputs to increase alarm accuracy. This industry also recommends turning off warning sensors when they are not needed (e.g., backup warning device turned off when the car is in drive). It also recommends that higher priority alarms override alarms of lesser priority to reduce interference. The nuclear industry recommends testing various alarm reduction strategies and system sensitivities to make informed decisions about what works.
Guidelines Applicable to the Auditory Modality. The automotive industry recommends that non-alarm noises produced by the system (e.g., radio or heating, ventilation, and air conditioning fans) be muted in the presence of auditory alarms. The aviation industry recommends that systems filter out environmental noises that could produce false auditory alarms.
Guidelines Applicable to the Visual Modality. The automotive and nuclear industries recommend that visual alarms be sensitive enough to warn users before a critical event occurs but not so sensitive that they produce frequent nuisance alarms.
Appropriateness
Guidelines Applicable to Visual and Auditory Modalities. All three industries recommend using bimodal alarms for critical information. The automotive industry provides guidelines for multistage alarms (i.e., alarms that occur sequentially over time) indicating graded warning levels. One-stage alarms should be used when immediate action is required or if a two-stage alarm may be considered a nuisance. Two-stage alarms are recommended to promote long-term behavior change or when urgency is less preferred (e.g., suddenly braking a vehicle in icy conditions is not the preferred response). Multi-stage alarms are recommended to provide continuous information (e.g., directions). The automotive industry also recommends that alarms be deployed after a trigger condition has been present for a predetermined time.
The aviation industry recommends bimodal alarms be used in environments with high ambient illumination, when auditory signals are nonverbal, and as needed to attract attention to visual alarms. This industry also recommends a single audio signal be used with multiple visual displays if locating the correct visual display quickly is not critical. The nuclear industry recommends the user be notified (modality not specified) when parameters are unexpectedly outside of normal conditions or when an expected parameter (e.g., status alarm) is absent. Additionally, once the user has cleared an alarm, the system should alarm (modality not specified) the return to normal conditions if it is important for the operator to know a deviation has been cleared. The nuclear industry also recommends that unacknowledged alarms be presented bimodally.
Guidelines Applicable to the Auditory Modality. All three industries agree that auditory alarms should indicate when immediate action must be taken and should be used when the system is not regularly monitored (e.g., when a workstation is not located in the main operating area of a plant). The automotive and aviation industries recommend that auditory alarms be used when the information is simple and short, when there are too many existing visual alarms for a particular workflow, and when the environment makes a visual alarm difficult to see. The automotive and aviation industries recommend that the type of auditory alarm (e.g., tone, speech) be chosen based on the specific situation. For the most part, the industries provide different, though not conflicting, recommendations; the automotive and aviation industries agree that tone alarms should be used in situations that require immediate action and speech alarms should be used to convey complex information.
The automotive industry recommends using earcons (e.g., “ding,” two chimes) to draw attention to cautionary alarms. Speech alarms should be used in situations where time is not critical since delivery of the alarm is longer than a tone; however, speech alarms may improve hazard detection and reaction time.
The aviation industry recommends using auditory alarms to remind users of actions to be taken, but not using them to indicate normal conditions. The aviation industry states that tone alarms are appropriate when used in combination with other alarms (e.g., flashing, text). Speech alarms are appropriate when a tonal alarm may be forgotten, when the ambient environment may mask a tonal alarm, or when presenting continuous information. The aviation industry recommends using auditory coding (i.e., alarm information that is conveyed by sound characteristic, such as high-pitch sounds for urgent alarms and low-pitch sounds for nonurgent alarms) for critical alarms, supplementing visual signals, providing feedback, and presenting information when a visual alarm is not possible.
The nuclear industry recommends using auditory alarms to indicate when a visual alarm is presented and a reminder tone to attract attention to the visual alarm that is unacknowledged. The nuclear industry recommends against using speech alarms to present complex information, when there is a memory component, when there are multiple alarms, or when special information is important.
Guidelines Applicable to the Visual Modality. The automotive industry recommends that visual alarms be used to deliver complex, lengthy messages in noisy locations or locations with frequent auditory alarms that the user continuously monitors. The automotive industry suggests that visual alarms are best at delivering information that needs to be referred to later or acted on immediately, or that deals with locations in space.
Context-Dependence
Guidelines Applicable to Visual and Auditory Modalities. The automotive industry recommends that auditory and visual alarms be easily perceivable in an environment. The nuclear industry recommends that alarms appear in locations where users who can address the alarm are likely to reside (e.g., send maintenance alarms to maintenance stations) and if an alarm type is relevant to more than one user group, it should be routed to all relevant group locations. Also, only users with visibility to the alarm and alarm information should be able to reset alarms. This industry also recommends that if alarms are separated from their source information (e.g., a red light indicates an alarm and an alarm log indicates the reason for the alarm), the alarm and the information should be physically close together.
Guidelines Applicable to the Auditory Modality. The automotive and aviation industries recommend that auditory alarms be distinguished from environmental noise. The aviation industry specifically recommends distinguishing auditory alarms in intensity, duration, source location, and frequency from the environment and recommends that auditory coding not be used in noisy environments. The aviation industry recommends that any speech alarms are distinct from other recorded speech in the environment (e.g., intercom communication). It also recommends that auditory alarms be compatible with clothing and equipment (e.g., headgear, hearing protection) and that alarms do not mask important feedback from the environment. The nuclear industry recommends that auditory alarms be audible and duplicated in any relevant workstation.
Guidelines Applicable to the Visual Modality. All industries recommend that visual alarms are physically located within the users’ workflow and line of sight, especially critical alarms (e.g., blind spot detection alarms on side mirrors). The aviation and nuclear industries recommend presenting system status indicators and alarms in different locations. These industries also recommend placing visual alarms near controls required to respond to the alarm.
Design Characteristics
Guidelines Applicable to Visual and Auditory Modalities. The automotive industry recommends designing all alarms in a simple and understandable way and making bimodal speech and text alarms redundant (i.e., speech and text to provide the same information).
The nuclear industry recommends maintaining an alarm log with time stamps to support event analysis. The nuclear industry also recommends designing alarm systems that are resilient, give prompt indication of system or component failure, can be regularly tested, have maintenance systems that minimally impact the performance of the user, require alarm signals to be disabled when taking an alarm out of service, and do not interfere with the user’s ability to act on the alarm. It recommends requiring manual reset when it is important for the user to know the condition has cleared, and an automatic reset should be available when numerous alarms are present. The reset function should return the alarm to an inactive state. This industry recommends changing alarms to a distinct acknowledged state (e.g., auditory alarm turned off, visual alarm changed color) after the user acknowledges the alarm. If a new abnormal range occurs, the alarm should be presented and distinguishable as a new situation.
Guidelines Applicable to the Auditory Modality. The automotive and aviation industries recommend specific frequencies and loudness for auditory alarms in general, in comparison to ambient noise, at specific distances, and in the presence of obstacles. These industries also recommend speech alarms be short and use formal language. The automotive industry recommends that speech alarms not be preceded by an alarm tone; however, the aviation industry recommends preceding alarm tones to speech alarms. The aviation and nuclear industries recommend designing alarms that will not startle the user.
The automotive industry recommends using high-bandwidth signals with a high signal-to-noise ratio, and a few distinct tones to discriminate between auditory codes. The automotive industry recommends speech alarms be natural voice or an easily understood synthesized voice.
The aviation industry recommends creating auditory alarms with two elements: an alarming signal (i.e., catches attention) and an identification signal (i.e., relays information). Additionally, avoid using midfrequency auditory alarms when they require localization. The aviation industry also recommends auditory alarms be designed to be clear, unambiguous, and understandable to prevent alarm failure. The aviation industry recommends using intelligible and descriptive speech, avoiding words that sound like other words, digitally processing speech to increase intelligibility, and using the North Atlantic Treaty Organization (NATO) alphabet (e.g., Alpha, Bravo, Charlie) for alphabetic information. The aviation industry also recommends using auditory codes that differ in two or more dimensions (e.g., pitch, temporal pattern). The aviation industry also recommends using brief and intermittent auditory signals rather than a continuous one and recommends specifications for the duration of auditory alarms. The nuclear industry recommends automatically resetting auditory alarms when they are silenced.
Guidelines Applicable to the Visual Modality. The automotive and aviation industries recommend avoiding certain colors in visual alarms and designing visual alarms so they are highly visible. The automotive and nuclear industries recommend that visual alarms be designed with high intensity, contrast, and luminance. The automotive industry recommends adjusting the flash rate to ensure the alarm is comprehensible, avoiding bouncing or zooming in visual alarms, limiting the number of colors in visual alarms, and using simple fonts and icons as well as minimal text.
The aviation industry recommends brighter, more saturated colors to draw attention and specific luminance contrasts between background and foreground in typical settings and in a dim state. The aviation industry recommends specific flash rates and flash coding on visual alarms, and that visual flashing alarms synchronize with one another and flash a symbol, asterisk, or arrow as opposed to the text or the whole alarm. The nuclear industry recommends specific flash rates for visual alarms and that if a flashing alarm fails, it should fail to an “on” position as opposed to an “off” position.
Mental Model
Guidelines Applicable to Visual and Auditory Modalities. The automotive and nuclear industries recommend that related alarms should be grouped together. The automotive industry recommends that for multimodal alarms, visual components should be presented to the user longer to maintain situational awareness. The automotive industry also recommends designing alarms that are easy to recognize and understand based on the user’s existing knowledge.
The nuclear industry recommends that alarm groupings should be based on naturally occurring relationships when possible. This industry recommends consistent formatting of alarms on all displays, including word order (e.g., title, value, severity), alarm arrangement (e.g., pressure placed above temperature), and alarm control arrangement (e.g., reset placed below acknowledge), as well as consistent terminology, symbols, and standards across alarm displays and procedure manuals. The nuclear industry recommends limiting aggregated alarms (e.g., single alarms that combine data from multiple sensors), but if aggregated alarms are used, users should be able to see which information is outside of normal conditions. This industry also recommends providing clearly labeled and usable aids for interacting with alarms and performing system maintenance, and a system design that enables user comprehension.
The nuclear industry recommends using minimal alarm coding strategies to make it easier to understand. It recommends separating controls for silencing, acknowledging, resetting, and testing alarms, and making these controls distinct.
Guidelines Applicable to the Auditory Modality. The aviation and nuclear industries recommend designing auditory alarms using few auditory codes, especially when users are required to identify the meaning of the alarm. The aviation industry recommends testing for system alarm usability using representative users. It also recommends avoiding operator confusion, errors, and inefficiencies when responding to auditory alarms and providing a consistent method for acknowledging alarms across the system. The aviation industry recommends keeping auditory alarms consistent across the system, using standard accents from the user’s country, utilizing existing associations for auditory alarms, and avoiding the use of sounds with old associations to represent new concepts.
Guidelines Applicable to the Visual Modality. The aviation industry recommends using symbols and icons as well as colors that utilize existing associations (e.g., octagon stop sign, yellow triangle). It also recommends maintaining consistent visual coding of alarms within the system and equipment. The nuclear industry recommends standard terminology and abbreviations for visual alarm titles and legends, and a single display area for high priority alarms.
Prioritization
Guidelines Applicable to Visual and Auditory Modalities. The aviation and nuclear industries recommend designing an alarm management system that prioritizes urgent and important alarms, and when two alarms appear simultaneously, the higher priority alarm is presented and the lower priority alarm is suppressed. The aviation industry recommends alarms be categorized into a limited number of priority levels with distinguishable characteristics. The nuclear industry recommends that high priority alarms be detectable under any expected environmental conditions.
Guidelines Applicable to the Auditory Modality. The automotive industry recommends that auditory alarms reflect prioritization through sound intensity.
Guidelines Applicable to the Visual Modality. The aviation industry recommends that the most important alarm information be displayed on the top left of the screen and the least important on the lower right. The nuclear industry recommends that if visual alarm information is displayed separately from detailed information, the detailed information should show the priority and status of the alarm. In the context of multiple alarms where some alarms are suppressed to address the priority alarm, once the priority alarm has been acknowledged, this industry recommends that alarms that may have been suppressed reappear.
Specificity
Guidelines Applicable to Visual and Auditory Modalities. All industries recommend designing visual and auditory alarms that are easily distinguishable from one another. The nuclear industry recommends that each technique used to code alarms (e.g., color, pitch, placement) should represent one aspect of alarm classification (e.g., color only represents priority). It also recommends distinguishing alarms based on their system state (e.g., unacknowledged, acknowledged, cleared).
Guidelines Applicable to the Auditory Modality. All industries recommend designing auditory alarms that are easily distinguishable from one another. The aviation industry recommends auditory coding that distinguishes signals based on the necessary response. It recommends that tone alarms are distinguished using intensity, pitch, beats, and harmonics, and that speech alarms are distinguished using different, distinct voices. The nuclear industry recommends designing auditory alarms that are distinct from other sounds produced by the system. It recommends using auditory codes that differ based on specified repetition rates and frequencies, but auditory codes should not use loudness as a dimension.
Guidelines Applicable to the Visual Modality. All industries recommend consistent visual coding of alarms using color, size, location, shape, and flash. The aviation industry recommends that system status indicators should be visually distinct from alarms. It also recommends using individual visual alarms to convey a singular message, except for master warning/summation lights. Additionally, warning/summation lights that summarize a subsystem should be visually distinct from their subsystem components.
Urgency
Guidelines Applicable to Visual and Auditory Modalities. All three industries recommend that alarms should indicate the degree of the problem they are highlighting. The automotive industry recommends using different modalities to signal urgency (e.g., visual for low urgency, auditory for high urgency). The aviation industry recommends using warning signals to indicate conditions requiring immediate action, while caution signals be used to bring awareness to certain unsafe conditions that do not present immediate danger.
Guidelines Applicable to the Auditory Modality. The automotive industry recommends matching the perceived urgency of the auditory alarm with the true urgency of the system and minimizing perceived annoyance, especially for low urgency situations. This industry recommends increasing perceived urgency of auditory alarms by using short and simple tones, fast regular rhythms that speed up over time, high frequencies, random overtones, large pitch ranges, atonal musical structure, obtrusive sounds, and more urgent words (e.g., danger). For speech alarms, the automotive industry recommends using a female voice and specific word rate to convey urgency. The aviation industry recommends using alarms that capture attention when the system requires high concentration from the user and repeating urgent auditory alarms until they are corrected or acknowledged.
Guidelines Applicable to the Visual Modality. All three industries recommend the use of visual characteristics to convey urgency, such as specific flash rates, bright colors, and high contrast, to indicate urgent situations.
The automotive industry specifically recommends the use of displays lit from the back (e.g., car warning lights) to convey urgent qualitative information. It also recommends using flash rates exclusively for situations that require immediate attention and using high flash rates for more urgent situations. The aviation industry recommends providing critical alarms if a user begins an action that could lead to danger or compromised data security, and these alarms should be interactive (e.g., ability to select yes, no, help) and prevent the user from interacting with the system until the alarm is acknowledged. The nuclear industry recommends using special coding to indicate urgency (e.g., all urgent visual alarms placed at the top of the display).
User Control
Guidelines Applicable to Visual and Auditory Modalities. The aviation industry recommends that users be able to request help when needed, have access to current alarm systems and shutoff switches, and be trained on alarms. For example, this industry recommends that users should easily be able to access suppressed alarm information. In some unspecified cases, the aviation industry recommends allowing users to set their own alarm parameters, but users should not be allowed to set alarm parameters when one user might affect settings of a second user or when parameters are determined by functional, procedural, or legal requirements. The aviation industry recommends automatically terminating and resetting alarms when the user performs the appropriate corrective action. The aviation industry recommends that any acknowledgment actions should not interrupt the user’s response to the alarm, and that users should be able to turn off noncritical alarms via the acknowledge button or turn off critical alarms once they have been acknowledged or corrected.
The nuclear industry recommends allowing users to access alarms that have been suppressed in favor of displaying high-priority alarms and subalarms that are nested in master alarms, and to see the current alarm parameters. Additionally, the user should be able to set temporary parameters that do not change the system parameters for specific conditions and should be required to acknowledge any changes they select. Parameters set by the system versus the user should be easy to distinguish, and system parameters should be under administrative control. Any automatic parameter changes made by the system should alarm the user and require user acknowledgement. The nuclear industry recommends designing alarms to prevent users from defeating the controls (e.g., intentionally placing a book on top of reset button).
Guidelines Applicable to the Auditory Modality. While both the automotive and aviation industries recommend that users control alarm volume and intensity, the aviation industry suggests that volume controls should be restricted to an extent to maintain minimum audible levels. However, the nuclear industry recommends no manual adjustment of alarm signal intensity.
Guidelines Applicable to the Visual Modality. The aviation industry recommends alarming the user if there is a loss of redundancy in the alarm system, and continuously displaying the lack of redundancy until the system is operable.