

Introduction
Central line–associated bloodstream infection (CLABSI) as defined by the Centers for Disease Control and Prevention’s National Healthcare Safety Network is a bloodstream infection (BSI) in a patient with a central venous catheter (CVC), without another attributable source of infection, that occurs when the CVC has been in place for more than two calendar days or removed the day before the BSI.1 In relation to other healthcare-associated infections (HAIs), CLABSIs are associated with an increase in patient morbidity and mortality and a high financial burden, accounting for approximately $46,000 per case.2
Cancer patients frequently require CVC for cancer-directed treatment, prolonged courses of intravenous (IV) antibiotics, and parenteral nutrition. The combination of an immunocompromised state and prolonged central venous access places patients at an elevated risk of developing a BSI.3,4 Development of a CLABSI prolongs hospitalization, causing an excess in resource utilization and treatment cost, and often delaying anticancer treatment, and is associated with a significant increase in mortality in cancer patients.5
An evidence-based bundle approach, in which a variety of clinical best practices are combined for insertion and maintenance of CVCs, has been documented in many studies and quality improvement projects.6–8 Adequate training, education, staffing, and leadership involvement are equally important standards in CLABSI prevention,9 as is the use of chlorhexidine (CHG) bathing.10 Removal of a central line when it is no longer clinically necessary is an important aspect of infection prevention. This is a careful consideration with cancer patients, as they receive important therapy through these lines. Additionally, the use of multidisciplinary central line rounds has proven to be instrumental in providing expert feedback to staff and gathering data.11
There are currently no reports in the published literature of virtual central line rounds being conducted. However, as care teams have grown and geographic coverage has increased, virtual technology has allowed healthcare professionals to connect when in-person options are not available.12 This virtual infrastructure has also strengthened as the COVID-19 pandemic ensued. New requirements for physical distancing, personal protective equipment shortages, and overtaxed inpatient medical and educational care prompted an inpatient virtual care model.13
Rationale and Current State
At our institution, nurses perform daily assessments and monthly audits of central lines to ensure alignment with a maintenance bundle. The bundle includes several components: assessing the line dressing and IV tubing, ensuring that disinfection caps are appropriately changed and secured, assessing if central line lumens remain patent, and verifying CHG-impregnated dressing was applied and CHG bathing performed. The care team also checks each shift for signs of infection, such as redness, pain, or swelling at the insertion site. Compliance with the bundle components is monitored by nursing leaders and reported on a monthly basis. Care teams have the ability to consult infectious diseases (ID) experts as needed.
In 2019, the medical intensive care unit (MICU) adopted a multidisciplinary model for central line rounding wherein a team rounded weekly to directly assess CVCs. The team included nurses, providers, and infection preventionist (IP) leaders. The term “provider” refers to physicians and advanced practice providers (APP), and APPs include clinicians licensed as advanced practice registered nurses, nurse practitioners, and physician assistants. The result of the MICU line rounds was a substantial decrease in CLABSIs from the previous fiscal year.11
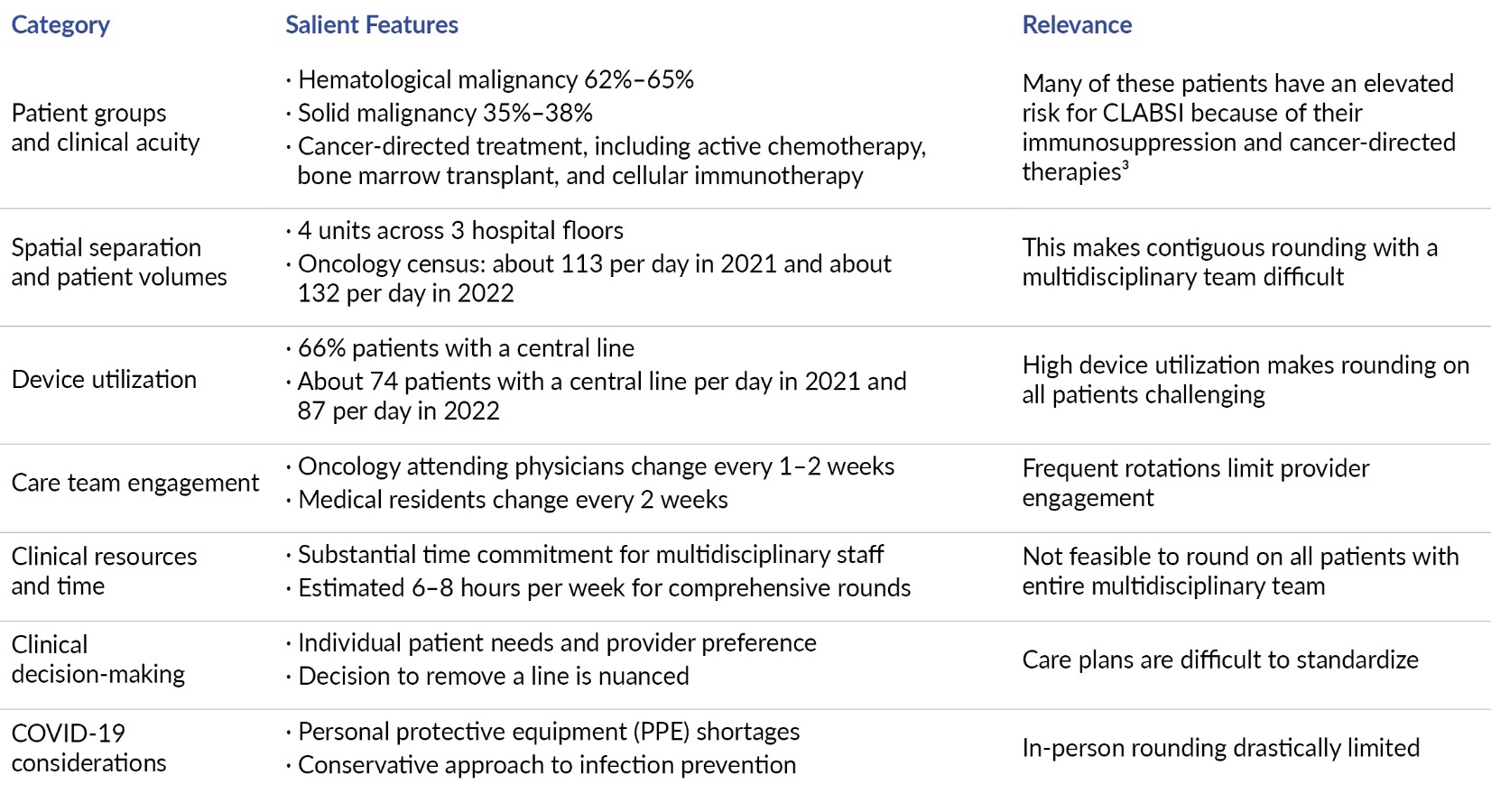
Driven by the success of the MICU initiative, we sought to adopt a similar model; however, there were several considerations specific to the oncologic population which informed the approach (Table 1).

Specific Aims
-
Design an interdisciplinary process for assessing central lines for risk factors contributing to infection, to counter challenges related to staffing, geography, central line volumes, and the COVID-19 pandemic.
-
Ensure the process allows for development of a plan of care to mitigate infection risk.
-
Reduce the CLABSI standardized infection ratio (SIR) by 10%, from 0.85 (November 2020–October 2021) to 0.77 in the 10 months after the intervention. The SIR is a ratio of observed infections to predicted infections, adjusted for facility and population-level risk factors.
Methods
Context
The intervention took place at a 910-bed tertiary care facility, part of an academic medical center and a six-hospitals-based health system in an urban center. The inpatient hospital oncology service cares for up to 144 patients across four units. The patient population is a mix of hematological and solid tumor malignancies, including bone marrow transplantation and cell-mediated immunotherapies.
Planning, implementation, and ongoing support was done by an existing oncology HAI subcommittee that meets monthly to tackle specific quality improvement efforts that align with hospital and system goals. The subcommittee is supported by an overarching clinical effectiveness team (CET), which steers and supports all aspects of inpatient quality and safety improvement efforts. The subcommittee is composed of ID and oncology physicians, APPs, clinical nurse specialists (CNS), clinical practice leaders (CPL), IPs, and a certified quality improvement advisor, all with a specialty in oncology. This group has existed since 2017, with CLABSI reduction as an ongoing focus.
In response to the barriers to in-person rounding described in the Rationale and Current State section above and with the additional infection prevention measures that interrupted in-person care due to COVID, there was a need to explore ways to support clinical review of central lines virtually. Looking to other areas where technology was leveraged to take the place of in-person clinical care, the group decided to use existing technology, a virtual platform, to fill the gap.
The choice to leverage existing technology allowed for quicker rollout of the intervention, limited training for staff, and required no purchase of additional technology with potentially lengthy organizational negotiations or approvals for use of a new platform. Additionally, the choice of developing this intervention within an existing platform allowed for smoother and quicker uptake by utilizing a mechanism that is already embedded in the culture of communication among staff.
Intervention
Summary of the intervention
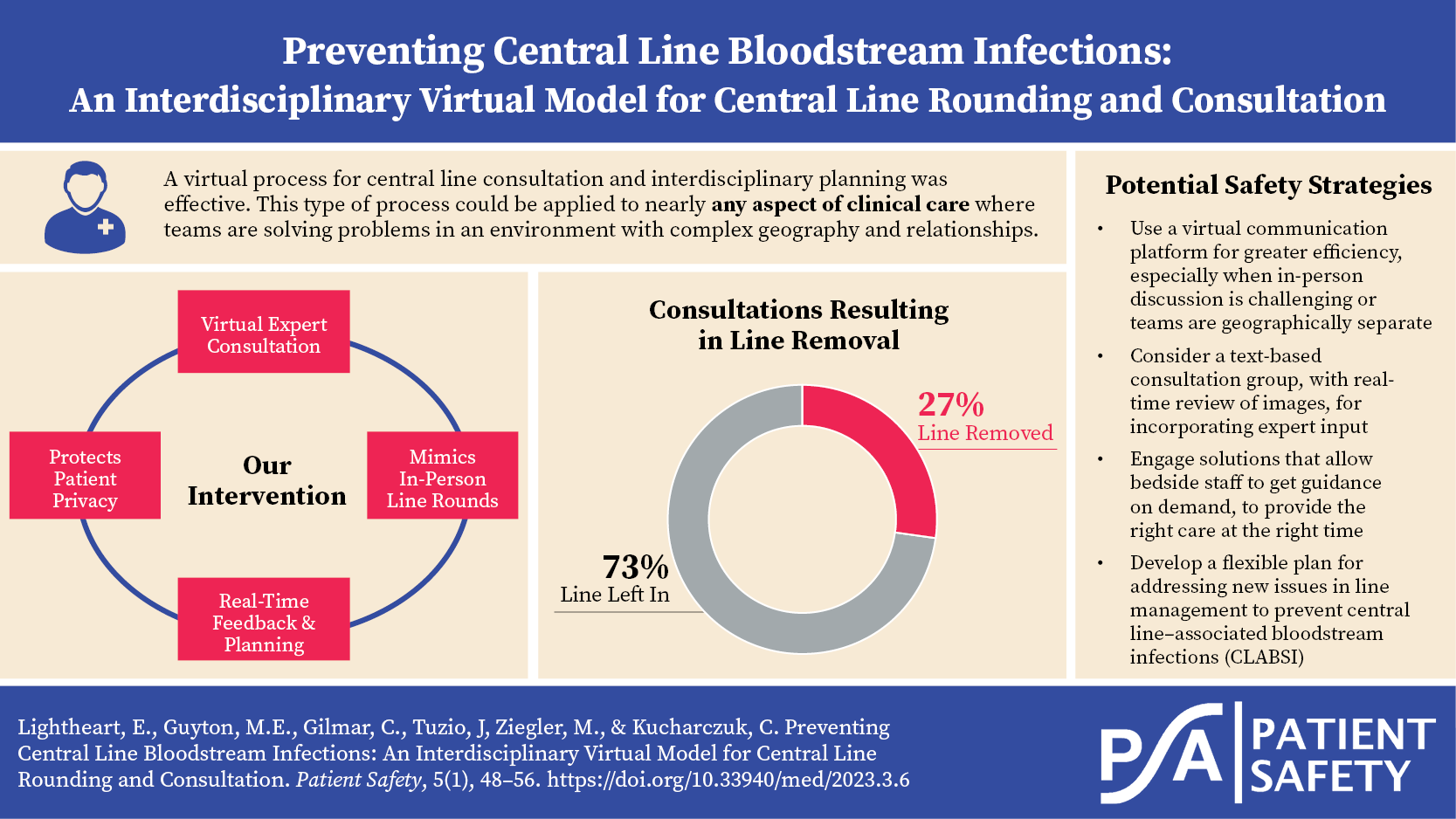
The project team designed a HIPAA-protected, virtual process for assessing central lines for risk factors contributing to infection. Staff initiated a consultation via virtual platform with an interdisciplinary team composed of oncology and ID experts. Line management recommendations were provided.
Throughout the intervention’s implementation, the team solicited feedback from users. Feedback was discussed at monthly HAI subcommittee meetings, and changes were incorporated through Plan-Do-Study-Act (PDSA) cycles.
Through a virtual platform, frontline oncology clinicians (nurses, APPs, physicians, IPs) sent a message to a receiving consultant group. This virtual consultation mechanism is called the Central Line Hotline (CL Hotline). The key consultants on the receiving end were members of the oncology HAI subcommittee with expertise in reducing CLABSI, including ID physicians, oncology APP leaders, CNSs, CPLs, and IPs.
The consultation could be placed by any clinician within inpatient oncology. Reasons why the consultation could be placed included concerning central line assessment findings (e.g., pain or tenderness, induration, significant erythema or concerning discharge); difficulty with central line dressings (e.g., line-site dermatitis, bleeding, adherence); issues with CVC maintenance (e.g., CHG bathing concerns); or clinical concerns for central line infection and consideration of central line removal (e.g., persistent fevers, bacteremia). The consultation message included central line assessment details, indication for the line, and a current photo.
Once the consultation was placed, the CL Hotline team reviewed the assessment findings and pertinent clinical data and discussed next steps directly within the virtual text thread. The receiving consultation group could add to or remove from the text thread any other members of the care team, as needed. The consultation team created an individualized plan of care for the patient’s central line. Meaningful aspects of care plans included the utilization of specialty central line dressings or products, administration of antibiotics, and central line removal. If the care team had not been part of the discussion up until this point, they were added to the virtual communication thread, and the plan was communicated to them then. Though members of the care team could arrange to meet at the bedside, this was not required, and all communication could feasibly happen virtually. After recommendations were made, nursing leadership and bedside nurses monitored the central line closely and consulted the CL Hotline again, if needed.

PDSA 0 (Pre-intervention) – Decision to focus on high-risk central lines
Before the CL Hotline’s conception, the project team decided to target its efforts on those patients whose central lines were considered at highest risk of developing a CLABSI. This included lines where concerns were identified during routine line care (e.g., line-site erythema, dressing concerns, or issues related to CHG adherence). This was driven by the oncology population’s particularly high volume of central lines. For several months, IPs, CNSs, and CPLs attempted to reach out to a small group of oncology infection prevention experts via email to discuss these high-risk central lines.
PDSA 1 (Primary intervention) – Decision to develop a virtual consultation process
1a. Choosing a virtual platform
Line evaluation via email proved cumbersome, as it was difficult to ensure the key people were included on each thread, and it was easy for emails to be missed or lost.
Additionally, the COVID-19 pandemic spurred an opportunity to address central lines virtually. A virtual platform was already widely embedded in patient care in the hospital units and easily adaptable for multidisciplinary consultations in the oncology units. Additionally, this texting platform allows for closed-loop communication, in which senders can see when and by whom messages have been read.
1b. Selecting the consultation team
The project team knew the consultation team needed to include representatives from across the inpatient care continuum—nursing leaders with extensive bedside experience and expertise caring for this population, APP leaders currently caring for hematological malignancy patients, ID physicians with specific expertise in oncology, and IPs focused on oncology infection prevention. As these stakeholders were all part of the oncology HAI subcommittee, a well-established and high-functioning team, the project group already knew their commitment to ongoing improvement in this area.
1c. Staff education
Prior to the implementation of the CL Hotline, education was disseminated to nurses, APPs, and physicians. Education included a one-page handout that was disseminated and discussed in various venues, including nursing huddles, staff meetings, and resident didactic sessions.
PDSA 2 – Increasing visibility and APP/resident engagement
One month into the intervention, the team received feedback from users that finding the correct group (the CL Hotline consultation group) was challenging. In response, the team worked with the organization’s communication colleagues to ensure the consultation group was viewable in the organization’s directory of consult services..The consultation criteria and goal of the initiative are listed within the directory.
The project team also sought to increase resident and APP engagement with the CL Hotline. The challenge here was that residents rotated into the oncology service every two weeks, with a new group of residents each time. So, additional education about the CL Hotline was incorporated into residents’ orientation onto the oncology service. Also, the hematological malignancy APP team incorporated regular progress updates in their staff meetings.
It is important to note that, at this time, frontline clinical nurses caring for patients were not directly consulting the CL Hotline. Those nurses were instructed to notify their nursing leaders (CNS, CPL, or nurse manager), who would consult the CL Hotline on their behalf. This decision was made to limit consultations to the CL Hotline because we were concerned that requests would surpass capacity.
PDSA 3 – Clarifying the nature of CL Hotline support
Five months after the initial implementation of the CL Hotline, the team learned of a lack of clarity about the longevity of support conferred by consulting the CL Hotline. Some staff assumed that consulting the CL Hotline meant their patient would be followed long-term by the consultant team, which was not the case. To address this, the team established a scripted response to be used as a reply to the initial consultation, so staff would understand that the consultation was a one-time intervention. Staff were asked to consult the CL Hotline again if new or lasting concerns arose.
PDSA 4 – Increasing nurse engagement, part 1
Eight months into the CL Hotline intervention, the project team sought to increase utilization by connecting into already existing processes within nursing. The team added a prompt into the device utilization tracking process to ask nursing leadership to consult the CL Hotline for concerning lines. At the same time, the team incorporated formalized education about the CL Hotline into orientation for new oncology nurses.
PDSA 5 – Increasing nurse engagement, part 2
Nine months after the start of the intervention, in further discussions about how to increase utilization, the team revisited the prior decision to have clinical (frontline) nurses reach the CL Hotline indirectly through their nursing leaders. The team agreed that not only could we accommodate more consultations, but also, more importantly, it would be beneficial for those closest to patient care to be able to consult the CL Hotline directly. The team did a new round of education with current clinical nurses about the change and modified oncology nurse orientation to reflect the change as well.
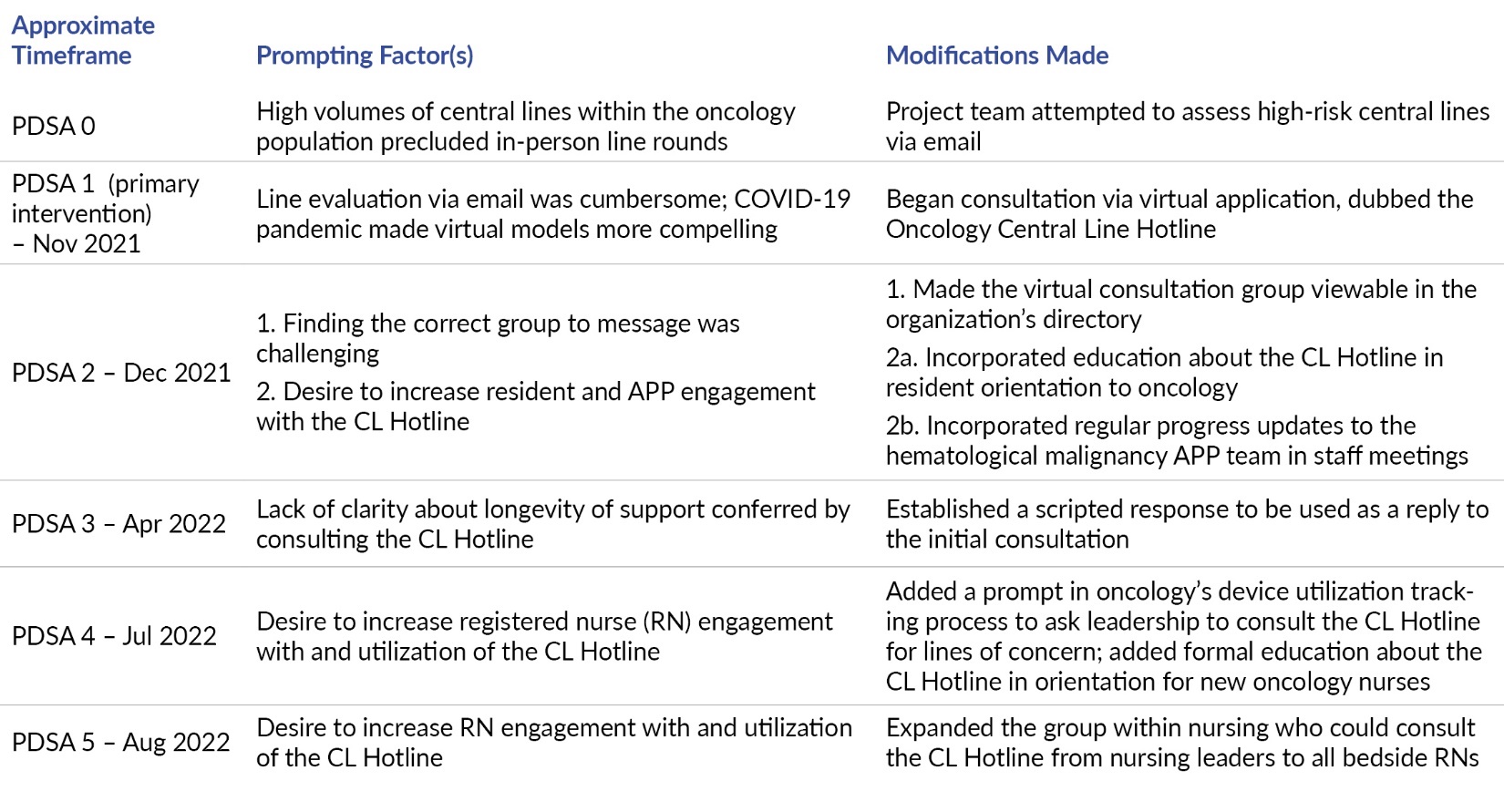
A summary and timeline of the team’s interventions and PDSA cycles is in Table 2.

Study of the Intervention
The project team used a Lean Six Sigma approach to assess the impact of the intervention, including the use of quantitative and qualitative data, Pareto charts, and run charts.
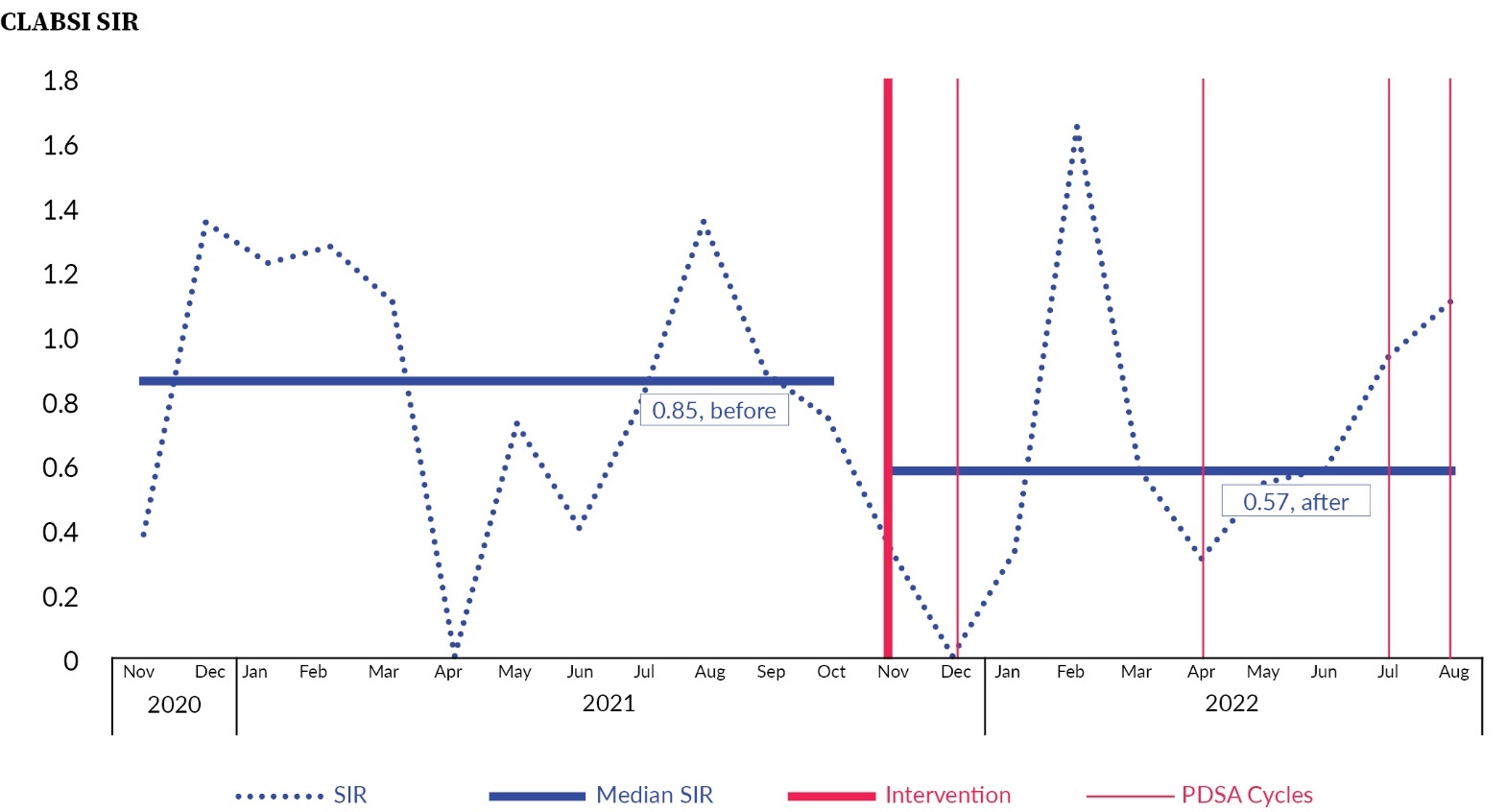
To establish whether the observed outcomes were due to the intervention, we plotted the timeline of interventions along the run chart for the primary outcome measure.
Measures and Analysis
The primary outcome measure we chose was the standardized infection ratio (SIR) for CLABSI, which is a risk adjusted measure which accounts for patient acuity and volumes. For process measures we tracked CL Hotline consultation volumes, line removal rates, and consult initiation by discipline and by unit.
We captured each instance of the intervention using an electronic data collection tool, collecting a selection of qualitative and quantitative data elements. We used Pareto charts to visualize the qualitative elements and to guide us toward adjustments in the PDSA cycles. We used run charts to gauge progress in the primary process and outcome measures, and to understand the effects of time as a variable.
The project team met regularly to review the data at a granular level, ensuring that those responsible for collecting the data understood the operational definitions of each data element and were capturing them similarly. To ensure the completeness and accuracy of infection data, we partnered with data experts within the Infection Prevention department. The team reported progress to an oncology-focused HAI subcommittee, who helped develop interventions and identify contextual elements that contributed to successes and failures.
Ethical Considerations
This quality improvement project was granted institutional review board exemption by the Human Research Protections Program, Office of Institutional Review Board within our institution. A HIPAA-compliant system was utilized to protect the privacy of the participants. Identifiable patient information was used for tracking and evaluation with a secure database. No data was collected directly from patients or families.
Participation from the consultative group and staff was voluntary and received no additional reimbursement for participation. Employees were invited to participate in the project voluntarily. Refusal of participation did not result in any punishments from the hospital leadership team.
Results
The CLABSI SIR has improved from 0.85 prior to the intervention (November 2020–October 2021) to 0.57 after the intervention (November 2021–August 2022) (Figure 2).

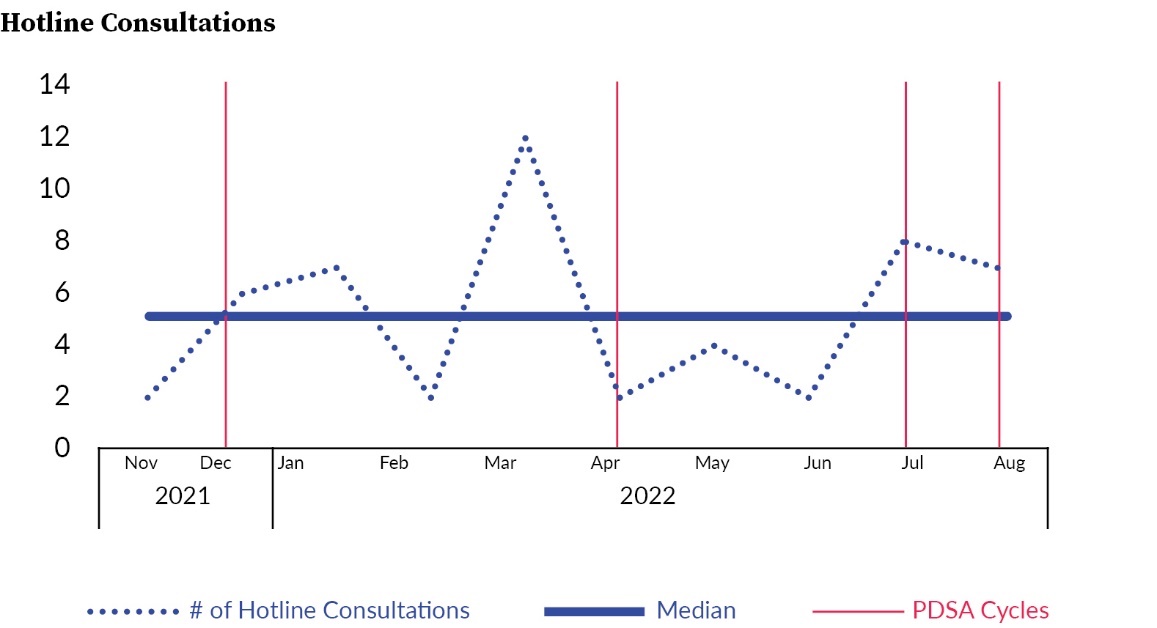
The number of CL Hotline consultations averaged about 5 per month. We were not able to identify what drove the unusually large number of consultations in March 2022 (Figure 3).

Of the 51 central lines cases submitted to the CL Hotline for consultation, 27.4% resulted in the central line being removed, which we believe contributed to the overall reduction seen in infection rates.
One substantive contextual element that may have interacted with the intervention is the opening of a new building within the hospital, which occurred at the same time as the intervention. All oncology units moved from their previous locations into the new building.
Anecdotally, communication and collaboration became more challenging in the new space, due to patient beds being spread out across larger areas and redesigned workspaces that sometimes resulted in providers being more isolated from nurses. The CL Hotline may have served as a tool to help mitigate some of these challenges.
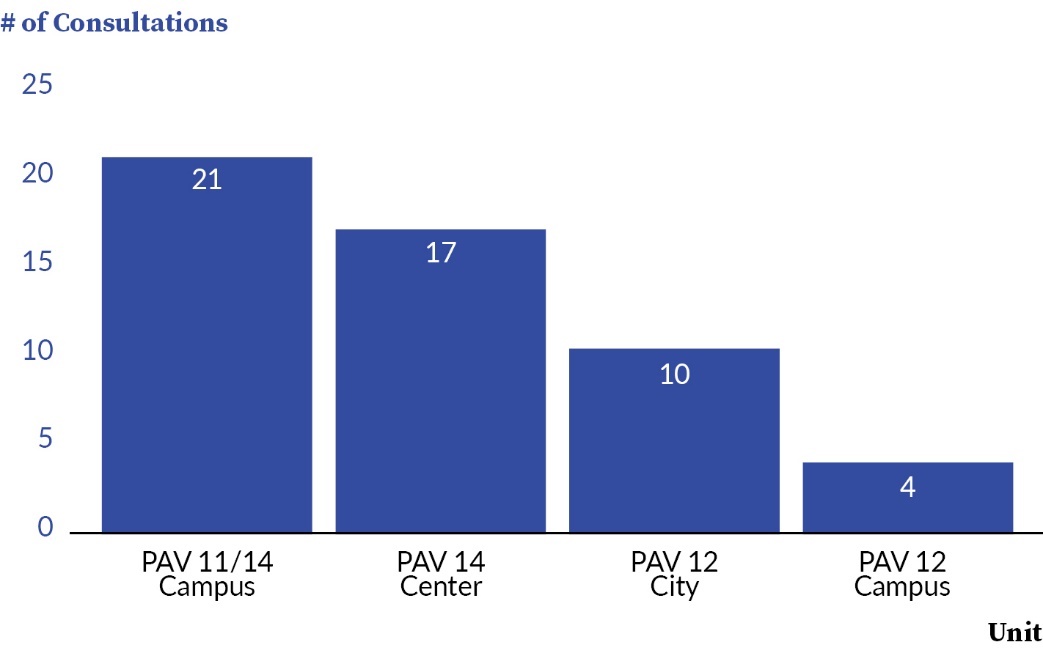
The hospital’s oncology units exhibited variation in consultation volumes (Figure 4), with the most frequent unit usage being five times that of the least frequent. This could be due to the mix of patients on the unit (fewer central lines), and to variation in how unit leadership emphasized the intervention. These results will guide future PDSA cycles to increase CL Hotline utilization.

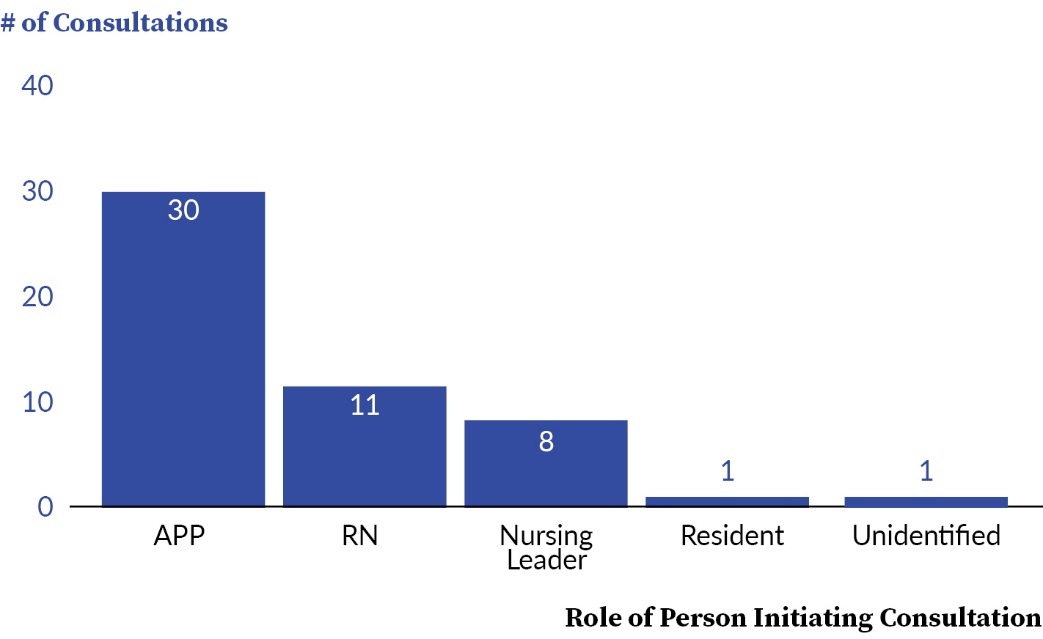
Additionally, as an academic medical center, many of the hospital’s patients were managed by resident physicians. Because these resident teams rotated onto the oncology service for two two-week periods at a time, it was challenging to establish a standardized process for these groups to consult the CL Hotline. Therefore, the project team focused initially on improving nurse engagement as a strategy, rather than resident engagement. These results guide future efforts to engage residents and other members of the care team (Figure 5).

Discussion
Interpretation
We found that after implementing a virtual line assessment tool
-
Staff utilized the CL Hotline and utilization volumes remained relatively consistent
-
Consultation to the CL Hotline facilitated the removal of lines which could potentially contribute to infection
-
The CLABSI SIR rate improved
The CL Hotline allowed the bedside clinicians to have a clear plan in place, individualized for the patient, after each consultation was completed. Advocating for central line removal can be overwhelming for staff members, and staff verbalized that they felt supported by the CL Hotline in this regard. The CL Hotline also expedited the management of site-specific concerns, such as dressing issues, to potentially decrease line-related morbidity.
The ability to share clinical details through photography, perform a virtual assessment, and produce an individualized care plan could be rolled out to other areas of practice. The CL Hotline had an oncology-focused lens, and expanding to a different patient population would require participation from other experts. This could be translated into many other areas where in-person rounding is challenging.
A limitation of the intervention was the hours of operation for the CL Hotline are only Monday through Friday during regular business hours. However, when the CL Hotline was not in operation, the medical team still had access to ID physicians, as normal and if needed. Additionally, our intervention was primarily reactive to issues and concerns brought up by the clinical care team and did not proactively identify issues. However, we believe proactive assessments are adequately addressed through other interventions, specifically central line maintenance bundles and central line audits.
Adapting existing technology had downsides. Using a prebuilt platform, the team was not able to customize features to support the particular intervention. For example, the virtual platform did not connect to our electronic medical record (EMR), preventing seamless linking of clinical information and the ability to automate documentation and follow-up actions. Unless a nurse or provider manually documented in the EMR that the CL Hotline has been engaged, this information was lost. A future goal is to explore options for integration into the EMR that would provide more streamlined communication between the CL Hotline and the patient’s care team.
Anecdotally, providers expressed concern that the CL Hotline would only lead to one outcome: the removal of the central line. In order to overcome this barrier, education was disseminated on the outcomes of the CL Hotline, which showed that line removal occurred only after 27.4% of the consults. Additional education was disseminated to discuss the other outcomes of CL Hotline usage, such as the utilization of specialty dressings, administration of IV antibiotics, and increased monitoring of the central line.
As reflected in PDSA cycle 5, changes were made to allow participation from bedside nurses. The team felt strongly about this shift to best address clinical needs and empower the nurses to participate when they identified concerns.
The team focused especially on striking a balance between increasing utilization and access to the service while maintaining capacity for the consult team to answer the volume of consultations. Consult team members participated in the service as an addition to their existing work and arrangements were made for coverage during time off. Since participation was voluntary and unpaid, expanding this service would be a challenge for the implementation team and likely would require participation from additional experts to share the volume of work. Capacity and membership of the core consultation group would need to be reassessed before planning expansion.
Limitations
The virtual platform did not allow for automated data collection. Collection was a manual process where information was entered into an electronic database by members of the project team. This manual process was more likely to generate measurement system errors.
The project team did not collect data related to education processes. It would be valuable to understand process measures related to staff education.
Conclusion
Utilization of a virtual platform is effective for multidisciplinary collaboration and support when in-person rounding is not feasible. Virtual consultative technology can be applied to other acute care settings where in-person rounding is challenging. The next steps are to improve sustainability by fully integrating the CL Hotline into the EMR.
Funding
M.J.Z. is supported by the National Institute of Allergy and Infectious Diseases (grant no. K23 AI143925) and CDC’s Epicenters for the Prevention of Healthcare-Associated Infections (cooperative agreement FOA no. CK16-004). The funding agency had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
Disclosure
The authors declare that they have no relevant or material financial interests.