Michelle Bell: Home medication management has not been a common research focus. What drew you to this topic?
Dr. Kathleen Walsh: That’s a great question. First, well one of the things is that I’m a primary care physician, so that’s where I see patients. Second, I’m a parent, so home is where I give my family medications. One of my first research projects was a four site study that looked at outpatient medication safety in children and adults with cancer. We found that the rates of medication errors in the home were quite high in children. In fact, the rate of errors overall in children was more than double that of adults with cancer: about 20% in children and 7% in adults, and it was entirely due to increased error rates in children at home. The rate of errors in children receiving chemotherapy infusion in the clinic was actually similar to adults.
There are two possible reasons for that: One is when pediatricians work with parents around medication use, we recognize that it can be challenging to get kids to take meds, especially kids with cancer. I think it’s a little easier to discuss that in pediatrics with parents so it’s more likely to be recorded in the chart. In addition, pediatric medication use is pretty complicated and error prone. So, it is more likely that they would have errors at home. Honestly, when I read the charts, I was struck by how incredibly hard this must be. They take 10 to 20 medications a day, they take multiple pills. It’s extremely complicated.
MB: We know how complicated the medication process is within facilities, where we have so much more control of the system. In the study,1 the research nurses used a four-pronged approach to find errors. Was any one of those more effective than another at identifying errors?
KW: The interesting conclusion from that study was that the rates of errors were extremely high, much higher than we had anticipated. Errors are ubiquitous with home medication use. And unfortunately, different methods discovered different errors. To find all the different types of errors, you need to use each method: observation, medication review, chart review, and parent interviews—the most effective being the chart review. It’s the easiest thing to do, but you miss important things if you’re only doing chart review. Some of the more serious errors were identified through parent interview and in-home medication review. For example, one family had moved and had a different concentration of oral chemotherapy at home than what the clinic chart had. So, they were giving a different dose than what the clinic thought they were giving. We were able to find that in the home because we looked at the bottle.

MB: Did any of the study results surprise you?
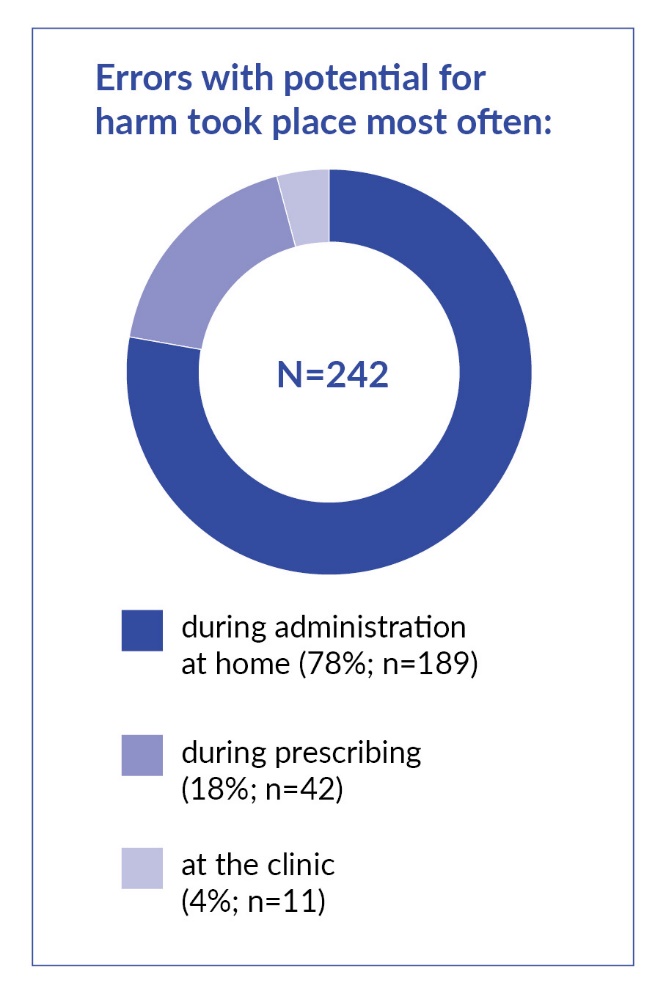
KW: Probably the most surprising thing in this study was how long errors in the home can last. In the hospital, most errors are intercepted before they reach the patient. In the home, if errors get to the point of administration, there’s no one to catch it. As a result, errors in the home went on for a long time.
MB: That’s consistent with what we see in acute care literature as well.
KW: Except the errors in the home may last for months, which differs from hospital care because more errors in hospitalized patients are intercepted before reaching the patient.
MB: You used the NCC MERP [National Coordinating Council for Medication Error Reporting and Prevention] harm scores to assess the actual outcome, along with severity scores for the potential worst outcome. Why did you choose to look at the possibility in addition to the actual outcome? And how do you differentiate between “significant,” “serious,” “life-threatening,” and “fatal?”
KW: Those terms [e.g., significant] were developed in the 1990s and are commonly used in safety research. “Significant” is generally any pain or a medically important change in your labs. For example, constipation, headache, an increase in your INR [international normalized ratio, which measures how long it takes for blood to clot] might be considered significant. “Serious” usually refers to more commonly known things like a pressure injury, a CLABSI [central line–associated blood stream infection], a serious medication error. We decided for this study, for example, that chemotherapy missed doses or underdoses are serious. Because children with leukemia need 90% 6-MP [6-mercaptopurine, an oral drug used to treat cancer] adherence, or they end up being at a significantly higher risk for relapse.
“Life-threatening” is very uncommon. For example, a hypoglycemic seizure in a child with diabetes would be considered life-threatening. Those decisions are made by two physicians independently, and we do assess inter-rater reliability for those. The NCC MERP worked pretty well.
MB: There were a lot of variations noted in the safety practices and cultures of facilities, and that’s something that we see as well when interacting with facilities—the difference culture makes. Did this influence the types of errors? I noticed site 1 reported more errors than sites 2 and 3 in the study. Was that due to culture or better identification?
KW: It’s not clear whether the detection was better at some sites than others or if rates of errors are higher at certain sites. There’s been a lot of work on how to maximize detection. I’ve never done a study without substantial site-to-site variation.
Sometimes the site with the highest rate prescribed the most medications. Once you address that, the rate goes down. In this study, that was not the case. The site with the highest rate also administered the largest number of medications, but when you accounted for the number of medications across the three sites, their rate was still highest. So, it’s hard to know for sure what the issue was. That site also had a lot of people that spoke different languages. But the types of errors were very similar across all the sites. I wish I could tell you. That would be an opportunity for collaboration between the sites to try to identify best practices.
But back to your question, you need to be able to benchmark right? You’re talking about a place we would love to get to, where there are measures that can be used by health systems to know the rate of errors for use in quality improvement to reduce it. It’s where we need to be in the next five years.
MB: Another challenge is quantifying events that didn’t happen. A student once asked me, “How do you get to a denominator? All the events that didn’t happen.” I told them that’s kind of like asking, “How many car accidents did you not get into on your way to school today?” Because the possibilities are so infinite as to where things can go wrong, capturing the potential failure points is almost impossible. How challenging is it to develop interventions in a system where you don’t have much control?
KW: We outline some in Table 4, but it doesn’t address everything that needs to happen. We developed it based on published research, but the field is evolving. Health system leaders need to recognize that they’re not just responsible for harm caused by healthcare within the walls of their hospital, but also that they share some responsibility when harm occurs from a medication prescribed in the hospital and administered at home.
Second, providers need to think about how well their plans can be implemented at home. For example, we visited the home of a teenager who was supposed to take 13 pills per dose, which sounds very difficult. I don’t know how the child did that. Sometimes children are prescribed things like 3.75 milliliters of a medication, which we would round. But parents may be uncomfortable just doing that on their own. At home, management of epilepsy, sickle cell, diabetes, and even asthma can be very challenging.
There’s a lot that we can do to help create a system that’s at least as safe at home as it is in the hospital for caregivers who aren’t formally trained. Parents are expected to give at-home medications where the dose on the prescription label is not the same as what they’re supposed to administer, which a nurse in the hospital would never do. This is because the dose has changed since it was dispensed. They would just send it back to the pharmacy to have it labeled properly.
Caitlyn Allen: How might the label that the parent sees differ from the one that was prescribed?
KW: There are a lot of medications that we have to titrate, meaning the doses go up and down to find the one that’s most effective. We titrate seizure medications, psychiatric medications, chemotherapy, steroids, hydroxyurea that we use for sickle cell. That’s just a few. The titration is a long process that parents often do in collaboration with their doctor. Take psych meds, which are common. If there is still medicine left in the bottle, the same bottle at home is often used even after the dose changes, so the label will often reflect the initial dose or some sort of attempt at summarizing how you titrate.
There have been many errors with this because it’s too complicated to try to follow the titration in your head. Or someone will follow the bottle label when it’s wrong, not follow the bottle label when it’s right. For kids with cancer, about 1 out of 10 meds at home has an old label on it and is not the current dose. That may be true for kids on psych meds or epilepsy meds as well. Does that help?

CA: That does. It’s really, really interesting.
KW: Yeah, it’s a big problem. If that happened in the hospital, no one would ever administer it. We’d just send it back. But it’s hard to figure out how to fix that problem. What you try to do is provide the dose on written material, then the family can kind of check it off. But everyone giving the medication in any setting has to have access to that.
CA: How often do pediatric doses change?
KW: Often enough. Back to the psych meds, if your child with autism is on antipsychotic medications, the doses in the beginning may increase. If there are side effects or the child grows, especially with weight-based meds, then the dose changes again. For example, even when we give kids regular Tylenol, the dose changes as they get bigger.
MB: What can facilities do today to prevent at-home medication errors?
KW: There are a few things. We’re working on measure development. Having a measure is the first step to quality improvement; health systems need to measure the problem continuously, then they can attempt different interventions to see if it improves. For example, you would look at central line–associated bloodstream infections or adverse drug events in the hospital. You measure them, then look for the reduction as you intervene. If you don’t have a measure, you won’t know if your interventions work and you won’t be able to benchmark performance. So, our top priority is doing a better job measuring outpatient medication errors. Right now, the best way to do that is through incident reporting in the ambulatory setting.
Once we have good measures, we can do a lot to try to intervene. Another thing providers can do is demonstrate how to measure the dose of a liquid medication with the family. Studies show that 100% of parents can accurately measure medications if you give them a syringe with a line on it and demonstrate the dose for them. Little things can help a lot.
The issue is for children on multiple medications, then they go home and have 10 different syringes. They need to attach the syringe to the bottle with a rubber band. That’s helpful. So is a written medication administration list. We should encourage using tools at home. We found in our research that among parents who don’t use any support tools with medications, 95% have errors. It’s less than half of that if they use something, a pill bottle, an alarm system, a calendar. I think the combination of system-level measurement and at-home safety tools are two places to start. Then just more innovation around what works to support families at home.

CA: Most of the time when we talk about medication errors, it’s related to the patient. This article discusses harm that can befall the person administrating the meds. Tell me more about that.
KW: This came up in our research for families using chemotherapy at home. You’re not supposed to touch oral chemotherapy. Publications from the 1970s showed that nurses managing these drugs developed urinary levels of the chemotherapy they were working with. Although parents are instructed not to touch the chemotherapy, most of them do anyway.
CA: How can parents protect themselves?
KW: They’re supposed to wear gloves and use pill cutters. The pill cutters are particularly important. A lot of parents don’t use them. They’ll break it with their hands. The problem is, if the child is taking a half pill a day and you break it off, it will likely crumble and result in a substantial difference in dose.
CA: Is using a kitchen knife a fair substitute for a pill cutter?
KW: Not really, no. Knives don’t work as well. Some pills are small, like an oral birth control pill. You can imagine, if you’re trying to cut that with a knife, it will crumble. Then your child gets less medication, and if the pieces are not cleaned up well others at home may be exposed to it. it. Plus, pill cutters are super cheap, or you can get a prescription for them.
We also don’t consider how safe or unsafe a medication at home may be in the same way we do in other settings. It’s hard to think that I’m giving something unsafe—or potentially harmful—to my child.
CA: Especially because it came from the physician, so therefore it has to be safe.
KW: Exactly, it can be counterintuitive. There are certain medications that are safe for anyone to take and others that are safe for one person and dangerous for another, based on your size, and how long you’ve been on it or whether you’ve titrated the dose.
CA: Is there any kind of guidelines for caregiver instructions?
KW: No, there isn’t really a standardized way that we talk to families about all medications. In fact, that’s one thing that we really need. I was never taught, “These are the things you have to tell a parent to administer a medication.” A standard approach would be helpful to give families expectations around the types of information they need to know when they receive a prescription. We’re working on standardizing conversations in the outpatient setting, so standardizing conversations around meds would be a really helpful thing to do.
CA: Speaking of improving conversations around meds, one of the more serious errors in the study was about a miscommunication between caregivers. Any suggestions about how to mitigate that?
KW: It’s funny you asked about that. We just accidentally overdosed my dog this week because of that problem. Fortunately, she was OK. My husband and I have made that mistake with our kids, I think because we both work. Often, one parent gives the dose, and then goes to work. The other parent doesn’t realize the first one gave the morning dose, and then gives it again. Or alternatively, one parent misses the dose, assumes the other one gave it, and the other also skips the dose, so no dose is given. It can be not just parents, but other caregivers as well. These double-dose errors at home are some of the most common errors.
Using a written tool addresses that. You write down a calendar that shows all the doses due while the child is on the medication, and you check it off when it’s given. Our problem this week with our dog was that I gave the medication but forgot to check it off on the calendar. So, written and verbal hand-offs help.
A similar error we also frequently saw was that one parent would go to the doctor and not tell the other about a change in dose. Then the other parent would give the old dose. That is particularly dangerous because it can go on for a long time, if the parents don’t regularly check in, for example if a parent is away or if they don’t live together.
CA: Could a patient portal help with that?
KW: A patient portal wouldn’t stop the double dosing with the two parents at home, but it may with the titration problem. My guess is often there’s one person who’s really in charge. Then they go away and the other is on over the weekend, and that’s when the communication failure occurs, or vice versa. Everyone may not have access to the portal as well.
CA: And like you said, the portal is only going to fix some of the problems.
KW: Exactly. I’ve known of parents of children with diabetes who are separated, who needed a dynamic solution, because diabetes requires regular, frequent checks throughout the day. So, they had an electronic tool that everyone could update in real time, the school nurse and both parents. That was pretty effective.
MB: I’m visualizing an app with an eMAR [electronic medication administration record] built into it.
KW: Yes, exactly. There are apps, but they’re not that sophisticated. If you’re on a lot of meds, and the doses are changing frequently, or the dose changes on different days of the week, the apps I’m aware of are not that good. Someday soon.
CA: Hopefully. Is there anything else that we didn’t cover, that you think would be important for folks to know?
KW: Medication errors in the outpatient setting, including at home, are common and dangerous—particularly for children with chronic conditions like cancer or diabetes, but even asthma or food allergy care can be complex and at times lifesaving. It’s important to remember that mistakes can happen and can have important consequences. But we can take basic steps to prevent these errors, such as prescribing doses that can be easily administered, trying to make sure that people know how to use their medications, and reducing the number of medications a child is on. Clinicians also need to recognize that the care we provide in clinic continues at home, and we influence that care. Whereas right now, at best we’re envisioning outpatient care as a hand-off rather than as a shared responsibility.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
Kathleen E. Walsh is a general pediatrician at Boston Children’s Hospital. Her research focuses on patient safety, particularly the safe care of children with chronic conditions in the outpatient and home settings. She has experience in the study of medication errors and adverse drug events among children in the hospital, emergency department, clinic, and home, and has developed health information technology interventions to support medication use. Dr. Walsh visited the homes of children with sickle cell disease, cancer, and epilepsy in single-site and multisite studies to understand barriers and facilitators of safe home medication use.
Michelle Bell is the director of Outreach and Education with the Patient Safety Authority (PSA). Bell began working with the PSA in 2010 as a patient safety liaison for Southeast Pennsylvania. She joined the PSA after completing a yearlong fellowship with the Institute for Safe Medication Practices, a world-renowned expert organization on medication safety.
Caitlyn Allen (caiallen@pa.gov) is director of External Affairs for the Patient Safety Authority and managing editor for Patient Safety, the PSA’s peer-reviewed journal. Before joining the PSA, she was the project manager for Patient Safety at Jefferson Health, where she also was the only nonphysician elected to serve on the House Staff Quality and Safety Leadership Council.