
Introduction
National awareness of patient safety risks has grown within healthcare since the report To Err Is Human: Building a Safer Health System by the Institute of Medicine (now the National Academy of Medicine) in 1999.1,2 Yet, the persistence of patient harm in our healthcare systems underscores weaknesses in our collective learning from adverse events; the challenges posed by siloed knowledge; and the lack of a positive, psychologically safe culture. The healthcare community increasingly recognizes the importance of creating an organizational culture that fosters collaboration and organizational learning and prioritizes patient safety instead of a culture of blame.
Rationale
From the inception of the modern patient safety movement, policymakers also recognized that organizational learning was a fundamental strategy for enhancing healthcare safety. The Berwick report strongly reaffirmed this viewpoint, aptly titled A Promise to Learn—A Commitment to Act.3 By embracing a culture of learning, transparency, and improvement, organizations can effectively learn from human errors and work towards improving safety and quality. However, the application of organizational learning in the healthcare sector has been relatively narrow.4
The National Steering Committee for Patient Safety recognizes the “learning system” as a foundational area for patient safety. This emphasizes a need to establish learning systems across healthcare organizations at local, regional, and national levels, fostering the development of safety learning networks.5
In the past decade, researchers, clinicians, and organizations have collaborated to create and implement network-based learning healthcare systems, termed learning networks, to spread learning broadly and rapidly with transparency.6,7 While researchers, clinicians, and organizations have created and implemented network-based learning healthcare systems, only a limited number of impactful and successful healthcare learning management networks have been documented in published literature.2,8
Goal
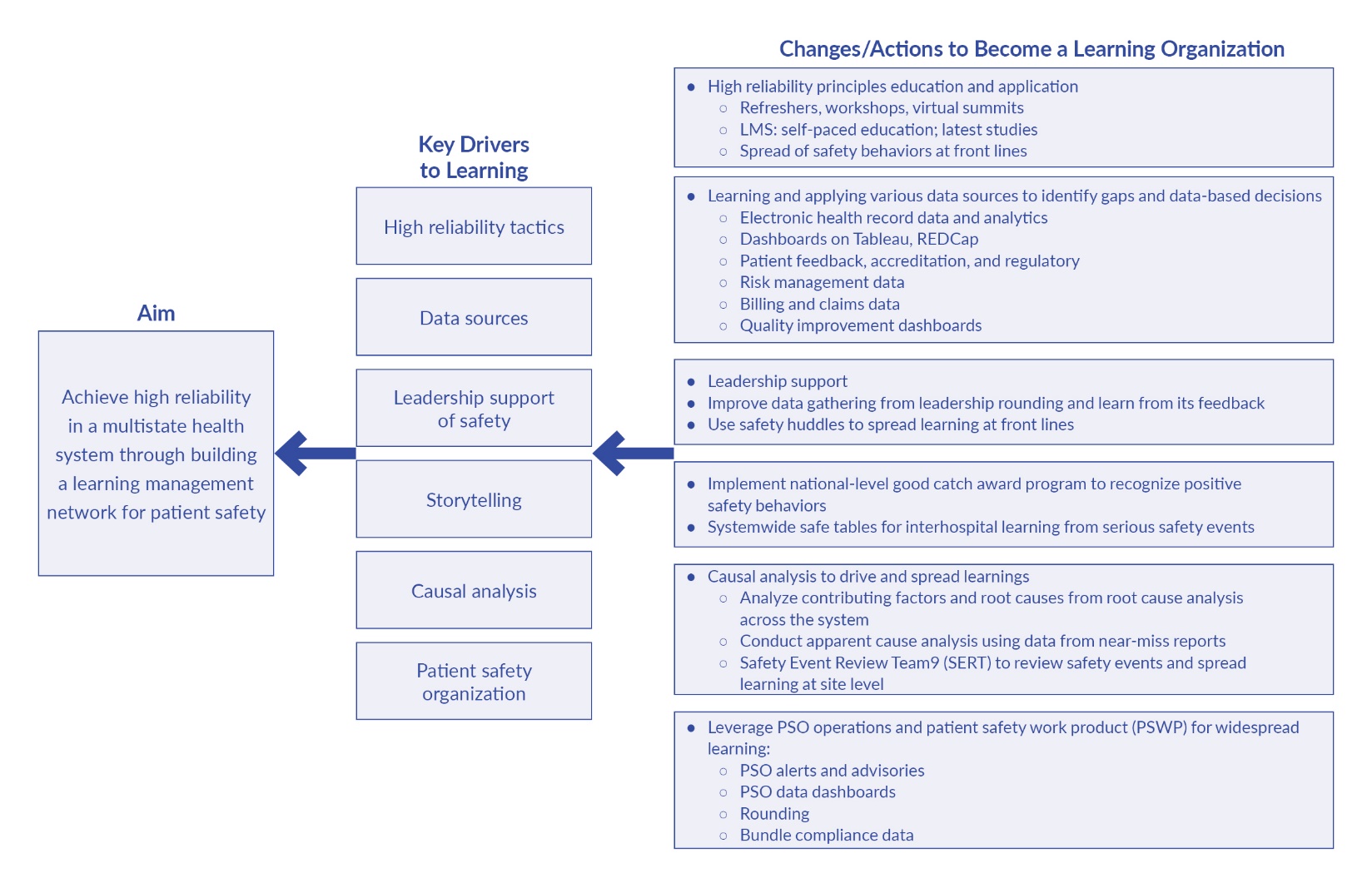
We aim to improve foundational measures of high reliability—patient safety event reporting and near-miss reporting rates—across Ascension, a multistate health system, by establishing a comprehensive learning management network dedicated to patient safety. This network will leverage key drivers for widespread learning, such as robust data sources, patient safety organization (PSO) resources, informed data analytics, storytelling, unwavering leadership support, and rigorous causal analysis. Through this initiative, we aspire to foster a continuous learning and improvement culture, ultimately enhancing patient outcomes and safety across all our facilities.
Our manuscript outlines a functional learning management framework’s formation, barriers, and early results. To our knowledge, our manuscript is the first to describe strategies for improving patient safety through the lens and framework of a learning organization, a foundational element for becoming a high reliability organization encompassing over 100 facilities across 12 states in the United States.
Methods
Context
In its commitment to enhancing patient safety and fostering a culture of excellence, our organization turned to the Safer Together: National Action Plan to Advance Patient Safety self-assessments to comprehensively understand the existing patient safety climate and culture.5 The analysis and discussion of the self-assessments’ results are beyond the scope of this paper. Still, in a nutshell, the assessments’ results affirmed that the foundation for enhancing patient safety lies in continuous and actionable knowledge generation. Simply collecting and reporting patient safety data falls short of the mark. Healthcare teams have a healthy appetite for learning from their sister sites, the types of events others experienced, what worked for others, and what didn’t.
An effective learning management network will address these learning needs and should begin to foster a psychologically safe environment where errors can be learned from and transformed into valuable lessons. Considering resource strains and ongoing economic recovery efforts, establishing an enterprisewide learning management network proved vital for efficient and widespread learning deployment.
Interventions
Guided by the “all teach, all learn” approach, we created a framework to share patient safety lessons across our network, highlighted by the key driver diagram in Figure 1. This roadmap, enriched by our history and the Institute for Healthcare Improvement (IHI) model for improvement, aims to fast-track learning and boost patient safety.9–12 The team that built and deployed this learning management network comprised national-level patient safety directors, certified patient safety professionals (CPPS), registered nurses with advanced degrees and several years of experience from several states, and educators. It was overseen by the vice president of Patient Safety and the organization’s chief medical officer (CMO).

High Reliability Principles Education and Application
We cater to busy healthcare workers with a customized learning management system (LMS) featuring the latest self-paced courses, simulations, and interactive tools with analytics-based feedback. This platform supports continuous education on new evidence and innovations, enhancing process, culture, and patient outcomes. This paper focuses solely on interventions related to patient safety.
To navigate the complex healthcare industry, we initiated a high reliability refresh to update our high reliability organizing (HRO) efforts. This included enhancing daily safety huddles, daily management systems, and leadership rounding to understand better and improve the current patient safety environment. Our training simplifies HRO principles for practical application, emphasizing human error understanding to develop strategies that reduce mistakes. Incorporating error prevention and safety behaviors is crucial to our refreshed HRO approach.
We use detailed facilitation guides for consistent delivery to maintain the quality of HRO training across 100-plus facilities. We’re expanding access to this training through virtual and self-paced online platforms, and our annual virtual patient safety summit further extends critical learnings to our entire workforce.
Learning From Data
Keeping a constant flow of data is essential for a complete picture of safety, like monitoring various dials for a complete view. Our incident reporting system is functional but captures only a portion of errors. Accurately tracking adverse events is vital, yet current tools have significant limitations. Even 25 years into the safety movement, organizations struggle to effectively assess safety program effectiveness and make meaningful comparisons between organizations.13–15 Our organization tracks harm rates and counts via our reporting systems, using rates for comparisons against benchmarks. Utilizing statistical process control (SPC) to monitor these rates helps identify specific vs. common cause variations, guiding our action plans.16 In some cases, understanding the impact of harm goes beyond benchmarks to humanizing data, focusing on affected individuals rather than abstract rates. It’s crucial to remember that real people are behind every patient safety statistic.
Beyond incident reports, process reliability audits and biannual safety culture surveys conducted by local teams and an external vendor are crucial for assessing safety practices and culture. Patient feedback, primarily through the electronic Patient Reported Outcomes (ePRO) program, adds a layer of accountability, allowing for direct input on medical status and experiences integrated into our electronic health record (EHR) system. A comprehensive risk management workflow supports this data spectrum, aiding in handling incidents, analyzing harm, and facilitating investigations. Leadership rounds and safety huddles also serve as vital data sources, offering real-time insights into safety practices.
Leveraging patient safety organization (PSO) privileges to share patient harm data across Ascension Healthcare PSO (AHPSO) facilities significantly boosts our safety efforts. Using Tableau, a software program with a user-friendly interface to enter data and view reports for daily updates on near misses, harm, and audits across all sites, gives us a detailed view of safety performance and improvement areas. We also recognize the importance of avoiding the “tyranny of metrics” and the pressure to measure everything for the sake of measurement, not improvement.17
Leadership Buy-in and Support for Learning Management in Patient Safety
Ascension’s leadership emphasizes building a culture prioritizing patient safety, ensuring a psychologically safe environment where staff can raise concerns without fear. Leadership fosters open discussions on errors and learning by eliminating the blame stigma. Both executive and clinical leaders are critical in visibly supporting this culture, providing resources, and removing obstacles to safety.
Two significant initiatives underscore the hands-on involvement of our leadership in supporting the learning management network for patient safety:
-
Firstly, leadership rounding has been revamped and made a critical priority within our organization. Leadership teams prioritize rounding with frontline teams and firmly schedule it as a recurring, non-negotiable event on their calendars. Designating “sacred time”—periods during which no meetings are scheduled, and time is specifically blocked out—ensures leaders have dedicated slots for conducting rounds. To bolster the effectiveness and consistency of these rounds, all leadership safety rounds are meticulously documented using the Ascension Rounding Tool (ART)—a valuable data source ensuring that insights gained and actions needed are systematically recorded and tracked for accountability and continuous improvement.
-
Safety huddles are considered a crucial two-way conduit of sharing and learning of safety threats and provide situational awareness for leaders, frontline managers, and bedside caregivers. Although daily shift huddles are not a new practice at our healthcare facilities, weekly market safety huddles set our organization apart. (A market is a geographical region with a cluster of hospitals.) A leader from the C-suite (usually a CMO or chief operating officers) owns these huddles, sends invitations, and ensures participation and accountability. A “look back, look ahead, and follow up” format is diligently followed at every huddle. The leaders participating in the huddles take the learning back to their people leaders in the hospitals, who then dissipate the teaching to their frontline associates.
Storytelling: Learning From National-Level PSO Safe Tables and Good Catch Award Program
National-Level Safe Tables
To enhance transparency and mutual learning across the organization, we introduced safe tables endorsed by The Joint Commission and Agency for Healthcare Research and Quality (AHRQ.)18 To ensure success with safe tables, we tackled two barriers. First, to overcome the geographical spread across 12 states, we used Google Meet, enabling easy access and dynamic interaction via polls and chat for widespread participation. Second, addressing concerns about blame and shame in discussing errors nationally, the vice president of Patient Safety engaged with local quality, safety, and risk management directors early on. They clarified the purpose of safe tables as a blame-free platform to share safety experiences and best practices, detailing scheduling and logistics well in advance to ready the organization.
After our inaugural safe table session in September 2022, those initial fears quickly dissipated, and we began receiving positive feedback through post-meeting surveys (see Results section). The experience demonstrated the power of this forum in fostering a culture of trust and learning, where the focus shifted from assigning blame to collectively improving patient safety. Our bimonthly safe tables, accommodating varied schedules, involve extensive preparation by patient safety, risk management, and quality teams, with input from executive leaders, managers, associates, and providers. Each session focuses on an in-depth analysis of safety events, presenting one or two cases using the Situation-Assessment-Background-Recommendation (SBAR) format. We use the Swiss cheese model to identify errors and lessons learned.12,19 Ultimately, we promote reflection on vulnerabilities and the need for action plan revisions, emphasizing continuous learning through PDCA (Plan-Do-Check-Act) cycles.
Learning From Storytelling: Good Catch Program
Storytelling, a potent tool in healthcare education and competency development, often surpasses traditional lectures in teaching safety concepts. Nurses frequently exchange stories of clinical successes, adverse outcomes, or near misses, highlighting the educational value of these narratives.20,21 We launched the Everyday Hero of Safety Award, a “good catch” program to capitalize on this, celebrate safety successes, and promote a proactive Safety-II approach.4,22
Launched in May 2021, our good catch program allows associates to nominate peers for their safety observations, fostering a culture of openness and encouraging reporting safety issues. A selection committee of safety, quality, risk management, and marketing experts picks a monthly winner based on criteria like the significance of the catch and the prevented harm. Winners are celebrated locally and recognized organizationwide via intranet and social media, promoting learning and acknowledging proactive safety measures. “Everyday heroes of safety” share their stories at our annual patient safety summit, emphasizing the importance of high reliability actions and a culture where speaking up is valued. Highlighting that good catches prevent adverse outcomes far more often than serious events, this initiative celebrates contributions, fosters teamwork, and encourages reflective learning.23
Learning From Causal Analysis: What Happened, Why, and What Can Be Done to Avoid Recurrence?
Analyzing significant safety events and preventable harm data revealed inconsistencies in our hospitals’ root cause analysis (RCA) processes and event selection. This analysis pointed out the need for standardized RCA methods, participant selection, and better sharing of RCA outcomes to enhance learning and improvement across the organization. To improve our Safety Event Review Team’s (SERT’s) approach, we standardized guidelines for event classification, team composition, and initial investigations. Inspired by Veterans Health Administration (VHA) and IHI models, we adopted a three-meeting approach for RCAs, separating interviews with involved individuals from larger RCA discussions to foster objectivity and focus on expertise.24–26 This method enhances learning, efficiency, and problem-solving while updating guidelines biennially with new evidence and practices.
We initiated a standardized RCA model through an in-person workshop, then switched to virtual sessions due to COVID-19 and resource constraints. To counteract the issue of isolated RCA insights, we adopted RLDatix, an electronic system for documenting RCA activities. This shift enabled detailed review of investigations, trend analysis of causal factors, and tracking of action plans, enriching our data use to prevent similar safety events. Coaching for RCAs improved, focusing on more robust action plans, with significant RCAs discussed at national safe tables.
Although RCAs are not new in our organization, we continue to face challenges, such as
-
Scheduling meetings for the RCA team is challenging due to healthcare staffing shortages, and we lack a robust solution.
-
The electronic documentation of RCA findings (to enable widespread learning) requires continual refinement, and we are currently researching technological solutions to streamline the process.
To mitigate low-to-moderate patient harm, our PSO member facilities required an alternative to the more extensive RCA process. So, we also adopted the apparent cause analysis (ACA), a limited investigation of near misses with fewer resources. Our electronic RCA documentation system provided a suitable platform for conducting ACAs.27,28
Our data does not fully show if RCAs prevent the recurrence of severe safety events without overusing resources. Recent studies have confirmed that many healthcare organizations’ RCA processes face the same problem, partly due to challenges similar to those we have outlined above.25
Using Our Existing PSO to Enable Widespread Learning
The AHPSO evolved from a data repository to a learning network for over 2,500 facilities across 12 states. Recognizing the value of PSO protections in 2019, Ascension employed Tableau for daily-updated safety dashboards and interactive reports, enabling data sharing in compliance with health laws. This facilitated knowledge-sharing through PSO alerts and advisories across the network, leveraging PSO protections to enhance patient safety learning across multiple states.
Measures
Our main objective in this improvement study is to enhance learning while balancing rigorous measurement and resource utilization. To achieve this balance, we planned to utilize the data in the event reporting system (ERS), enabling us to monitor our progress and determine if we are heading in the right direction. Associates throughout Ascension can enter patient safety events into the ERS. All events are then categorized on a scale of A–I, based on the National Coordinating Council Medication Error Reporting and Prevention (NCC MERP) index, where A incidents are “No Error, No Harm – Good Catches,” B–D are “Error, No Harm,” and E–I are “Error, Harm.”29 In this project, we employed the overall reporting rate, which includes all categories, and the near-miss category, which includes A–D severity levels. Both rates are determined by dividing monthly counts of event reports (numerator) by patient days (denominator) with 10,000 as a multiplier.
We did not initially plan to use the culture of safety survey data, adapted from AHRQ’s Surveys on Patient Safety Culture (SOPS).30,31 However, during the project, we noticed that one of the survey items, “Communication about errors,” is relevant to the goal of this project, which is to promote transparency and sharing of patient safety events. The “favorability rating” is calculated by taking the number of respondents who gave a rating of 4 or 5 on a scale of 1 to 5, with 1 being least favorable and 5 being most favorable (numerator) and dividing it by the total number of respondents (denominator).
Statistical Analysis
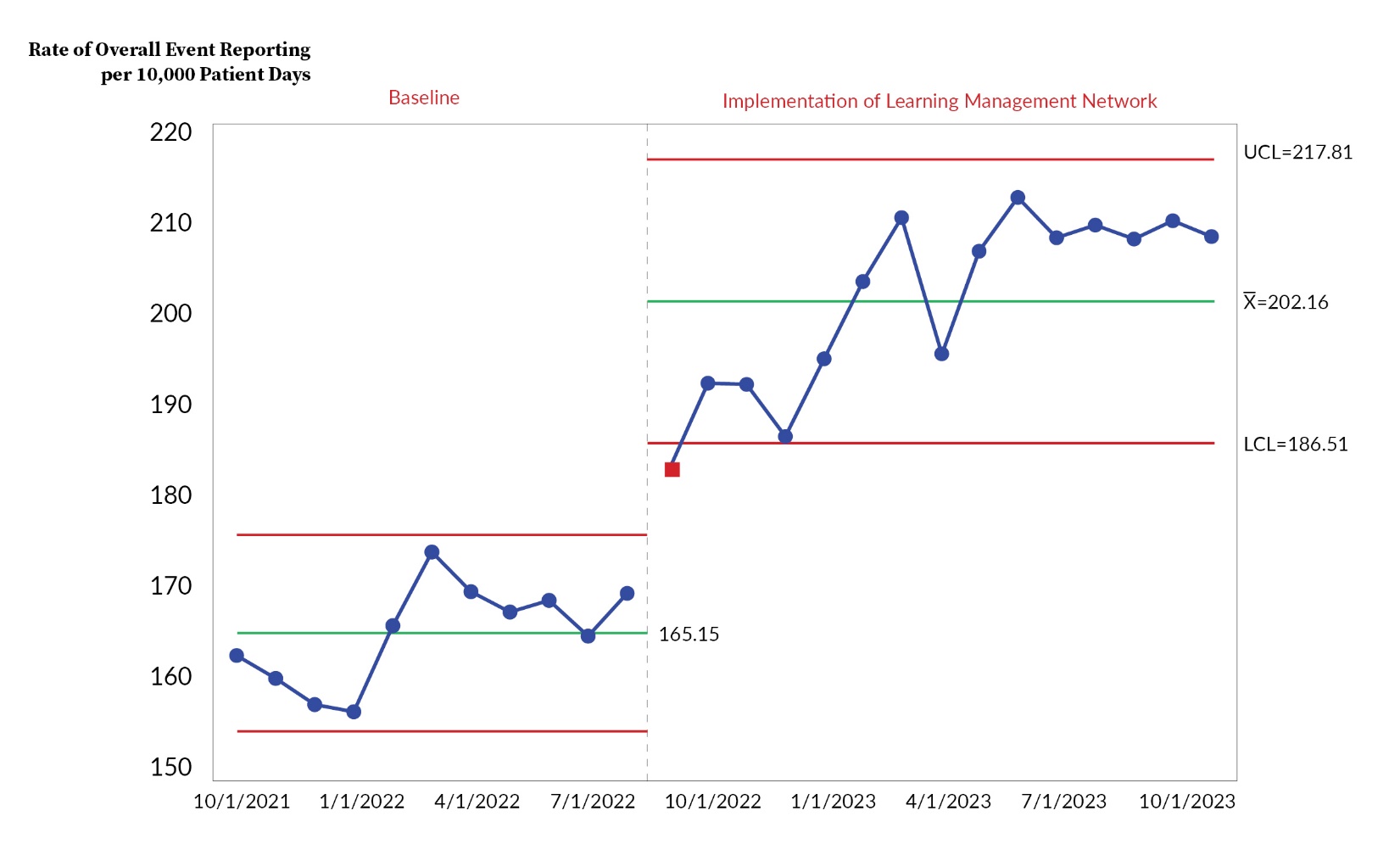
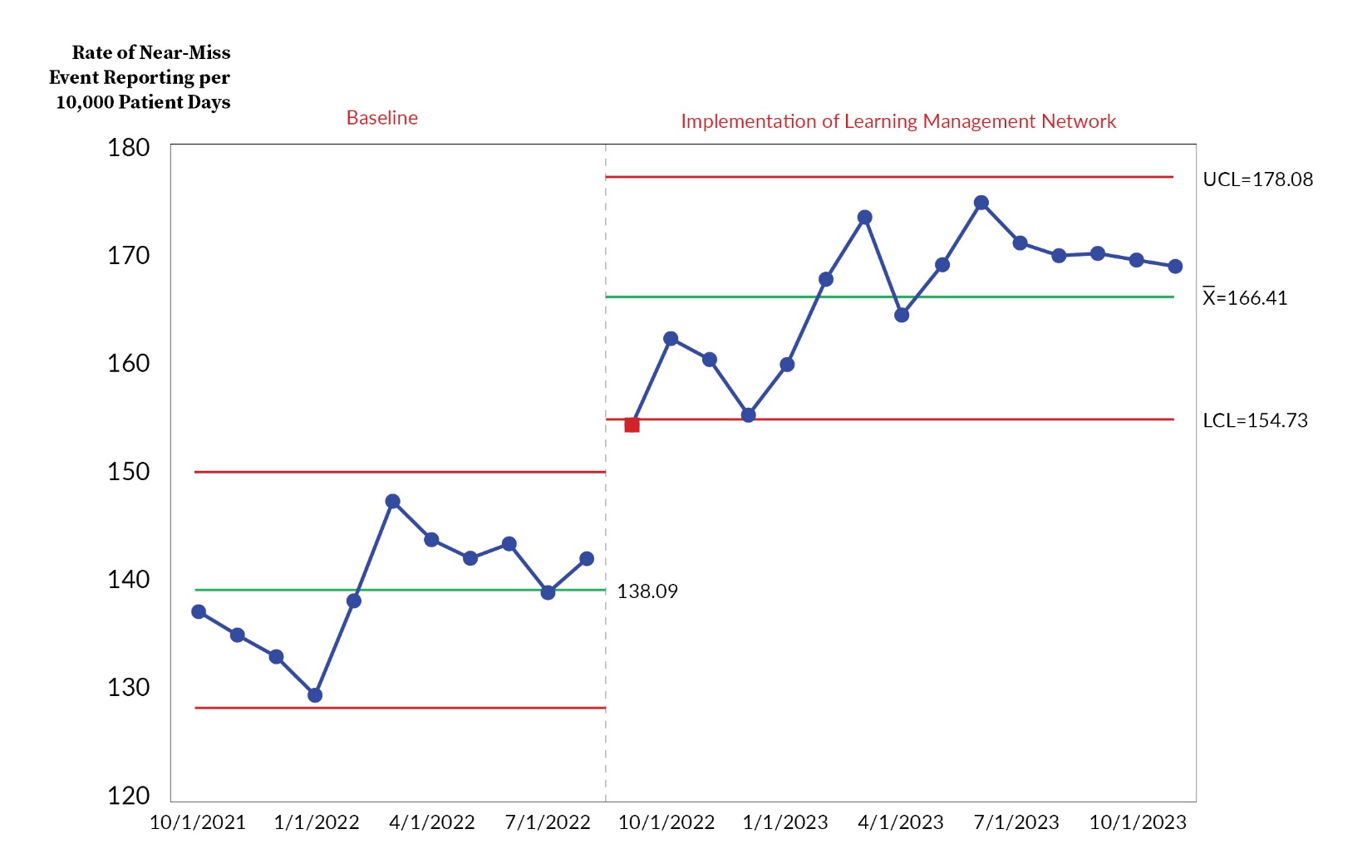
We utilized SPC charts (Shewhart charts) to display and evaluate our progress systematically over time.16 The two control charts used in this project are u-charts. They are generated using Minitab statistical software (version 21.1.0) and are specifically used to display and study rates—data with Poisson distributions. Both control charts have upper and lower control limits around the process mean (center line), displaying plus or minus three standard deviation from the process mean. Additionally, our data scientists conducted two types of hypothesis testing using Minitab to calculate p-values to establish statistical significance. We used a two-sample Poisson test to calculate p-values for the event reporting rate data sets and a two-proportion test for the “% favorability rating” data set.
Results
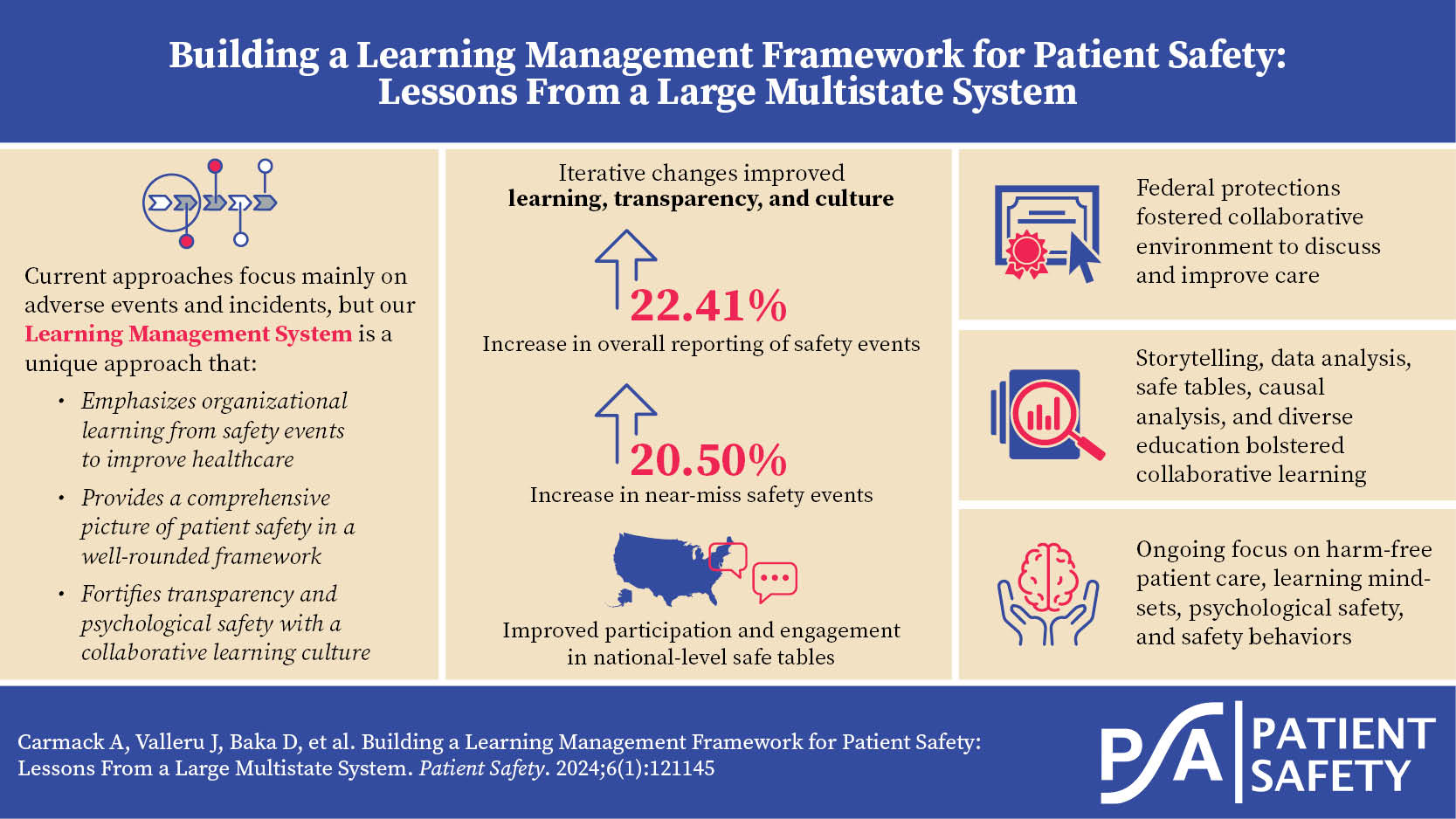
Our overall event (incident) reporting rate (Figure 2), which includes all severity levels of harm, increased from 165.15 events to 202.16 events per 10,000 patient days (p-value<0.0001), a 22.41% increase from the baseline period of 2021 to 2023. More importantly, the “Near Miss” and “No Harm” event reporting rate (Figure 3) also steadily improved across all regions and facilities from 138.09 events to 166.41 events reported per 10,000 patient days (p-value<0.0001), a 20.50% increase over the same two years. We hypothesize that the increased reporting rates, both overall and near miss, illustrate the influence of our widespread sharing of harm data and improved culture of transparency and learning being attained through the learning management network as described in the Methods section.


Although not part of the original measurement plan, we observed that in the culture of safety survey, the “Communication about error” survey element received a favorable rating of 70.6% (41,809/59,219) in 2022, representing an increase of 1.1% (p-value<0.0001) from 69.5% (39,928/57,450) rating recorded in 2020. Although a modest increase, it also suggests that our organization is moving toward improved communication about errors and a willingness to share and learn from errors at the front lines.
We routinely collected feedback from over 1,000 PSO safe table participants from all facilities as a qualitative measure. Some of the reflections were “I appreciated the respectful atmosphere,” “I really respect the ability to acknowledge where better decisions could have been made honestly,” “supportive of associates in the situation without pointing fingers,” and “The supportive conversation facilitated a safe learning environment.”
Discussion
We have faced various challenges during our three-year journey, which is still in its early stages, to establish a well-rounded learning management network to fortify patient safety. We have had to make multiple adjustments, but we are seeing some early indications of progress regarding our ability to learn, transparency, and culture. Notably, an increase of 22.41% (p-value<0.0001) in the overall reporting of safety events and an increase of 20.50% (p-value<0.0001) in near-miss safety events indicate that our patient safety community is more open to sharing and learning from each other, without fear of blame. We also observed that participation and engagement in national-level safe tables have greatly improved. AHPSO member facilities engage in healthy dialogues to share and learn from one another’s serious safety events and improvement strategies. These positive changes are anecdotal, yet they serve as an indication of the impacts of our intentional focus on learning management for patient safety.
Since the inception of the patient safety movement, healthcare has consistently acknowledged the pivotal role of organizational learning in improving the safety of care.32–34 Nevertheless, the prevailing emphasis in many current healthcare organizational learning approaches is primarily on adverse events and incidents. To our knowledge, our learning management network is unique in that it is a well-rounded framework that provides a comprehensive picture of patient safety and can infiltrate all levels of the hierarchy with rich and actionable knowledge, promoting a collaborative learning culture and a platform for continuous improvement.
Limitations
One of the challenges we face is ensuring that patient safety knowledge is disseminated effectively to all frontline users. For example, occasionally, we find that potential safety threats were discussed in a safety huddle, but they were not passed down to the next shift or to float nurses, resulting in a safety event. Another area where we can improve is the network’s ability to proactively identify and address system and process issues to prevent patient harm rather than reacting after an error has occurred. It is crucial that we address these limitations to maximize the effectiveness of our learning management network, further our commitment to patient safety, and become an effective learning organization. Furthermore, the level of transparency within the network has matured gradually and constantly requires substantial perseverance and patience.
This article outlines a framework for a collaborative learning network within a parent organization protected by PSO privileges, noting that networks across facilities with different parent organizations may operate and look differently. Collaborative patient safety campaigns led by IHI could serve as a model for organizations to form a learning network.35 Establishing a safety culture and a learning network is resource-intensive and funded internally by our organization. Detailing the specific costs of building and deploying this network is beyond this article’s scope. As our focus on patient safety evolved, we increased human resources and adjusted allocations to support the learning network’s expansion. Finally, a perennial challenge our multistate health system across 12 states faces is the potential for distraction by the constantly changing landscape of healthcare, competing priorities, post-COVID recovery efforts, staffing shortages, patient satisfaction, and varying state-level regulations.
Next Steps and Conclusion
Over the past three years, our primary focus has been on developing the infrastructure and addressing gaps in learning and sharing information within our PSO member facilities. Our goal is to instill essential learning mindsets, create psychologically safe workplaces, and promote high reliability and safety behaviors throughout the organization. While we have noticed progress in safety culture and transparency, we have yet to witness significant and sustained improvements in patient safety outcomes, specifically in reducing serious harm rates. Given our leadership’s unwavering focus, allocation of resources to patient safety, and improving incident reporting rates, we remain cautiously optimistic that we will decrease harm rates as our learning management network continues to mature. Our learning network across 12 states enables seamless knowledge sharing, highlighting the benefits of storytelling, data analysis, and diverse education in promoting collaborative learning. As we navigate the evolving healthcare landscape and aim for harm-free patient care, we focus on cultivating learning mindsets, ensuring psychological safety, and enhancing safety behaviors.
Author Contributions
AC: Conceptualization, Methodology, Supervision, Writing-Original Draft. JV: Writing-Original Draft, Formal Analysis, Investigation. DB: Investigation, Writing-Original Draft, Writing-Review & Editing. MH: Investigation, Writing-Original Draft, Writing-Review & Editing. SM: Investigation, Writing-Original Draft, Writing-Review & Editing. JW: Investigation, Writing-Original Draft, Writing-Review & Editing. KR: Conceptualization, Methodology, Supervision, Writing-Review & Editing.
Disclosure
The authors declare that they have no relevant or material financial interests.
About the Authors
April Carmack is senior director of Patient Safety at Ascension.
Jahnavi Valleru (Jahnavi.valleru@ascension.org) is program director of Patient Safety at Ascension.
DeeDee Baka is director of Patient Safety at Ascension.
Meghan Henderson is a patient safety manager at Ascension.
Sarah McCarter is a patient safety manager at Ascension.
Jeanene Walsh is a program manager at Ascension.
Kelly Randall is vice president of Patient Safety at Ascension.