Introduction
Patient safety event reporting is a cornerstone of healthcare quality improvement. Systematic documentation of adverse events, near misses, and unsafe conditions enables organizations to detect patterns, conduct root cause analyses, and implement targeted interventions to prevent future harm.1,2 Since the landmark report To Err Is Human, incident reporting has been recognized as a central pillar of safety culture, driving learning and system-level improvements.3 To enhance the standardization and comparability of event data, some national organizations have developed common formats, further supporting local and national safety initiatives.4 However, despite these advances, clinician-driven event reporting faces significant limitations.
Clinicians, particularly physicians, often underreport safety events due to barriers such as fear of litigation, punitive responses, time constraints, lack of feedback, and a persistent culture of blame.5–8 Nurses tend to report more frequently than physicians, but underreporting remains a widespread concern.3 The creation of a nonpunitive, confidential reporting environment with clear feedback mechanisms and visible action is essential to fostering a just culture and enhancing staff engagement.9–11 National organizations such as the American Academy of Pediatrics and the American College of Emergency Physicians have emphasized the value of reporting not only adverse events, but also near misses and unsafe conditions as a strategy for system learning and improvement.10
Beyond clinician-generated reports, there is increasing recognition of the value of patient and family contributions to safety surveillance. Patients and caregivers often detect communication breakdowns, procedural deviations, and harm that may go unnoticed by healthcare staff.11–13 Studies show that patient- and family-reported adverse event rates frequently exceed those captured through traditional reporting systems and often identify unique preventable events, particularly related to medication safety and interpersonal communication.14–16 Moreover, these reports seldom overlap with clinician-generated ones, further underscoring their complementary value.17
Systematic reviews support the impact of patient and family engagement on safety outcomes. Interventions that promote such engagement, ranging from educational materials to real-time technology platforms, have shown potential to improve detection of safety threats and reduce harm.2,18,19 Tools such as mobile apps and digital portals have demonstrated feasibility and increased reporting volume, though disparities in access and participation remain a concern.12 Importantly, qualitative studies emphasize that patients and families value the opportunity to be heard and meaningfully involved in safety efforts. Their participation in adverse event reviews can foster organizational learning, reconciliation, and trust in the healthcare system.20–22 Accordingly, professional guidelines recommend that families be engaged at all levels of care, including in safety reporting and event review processes.10
Despite this growing body of evidence, the implementation and evaluation of patient- and family-initiated reporting systems remain limited. Barriers include a lack of awareness, cultural norms, variable institutional support, and minimal integration into existing reporting structures.23–25 Most engagement efforts are focused at the direct care level, with relatively few system-level strategies in place.2,24,26 Although there is strong support among patients and families for engagement in safety processes, actual participation is shaped by structural supports, staff attitudes, and perceptions of legitimacy and role.27
While several prior systematic reviews have examined related domains, such as general patient engagement in safety, medication-specific reporting, or broad incident reporting processes, they have not focused specifically on patient- and family-initiated safety event reporting systems as distinct mechanisms within safety surveillance. This scoping review therefore aims to refine and extend the existing evidence base by mapping the characteristics, implementation strategies, reported outcomes, and barriers of systems explicitly designed for patient or family reporting across diverse healthcare settings. In doing so, it highlights how these systems function, where they diverge from clinician-led reporting, and what structural and cultural barriers shape their impact.
Methods
This scoping review followed the framework established by Arksey and O’Malley28 and was refined according to the methodological guidance by Levac et al.29 The review process was reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.30 The central research question guiding this review was “What is known about the implementation, use, and impact of patient- and family-initiated safety event reporting systems in healthcare?”
A comprehensive search strategy was developed in collaboration with a medical librarian. The databases MEDLINE (via PubMed), CINAHL, Embase, Scopus, and PsycINFO were searched using a combination of terms related to patient or family reporting (e.g., “patient complaint,” “family report”), safety events (e.g., “adverse event,” “medical error”), and healthcare settings. The search covered studies published from January 1, 2000, to May 10, 2025.
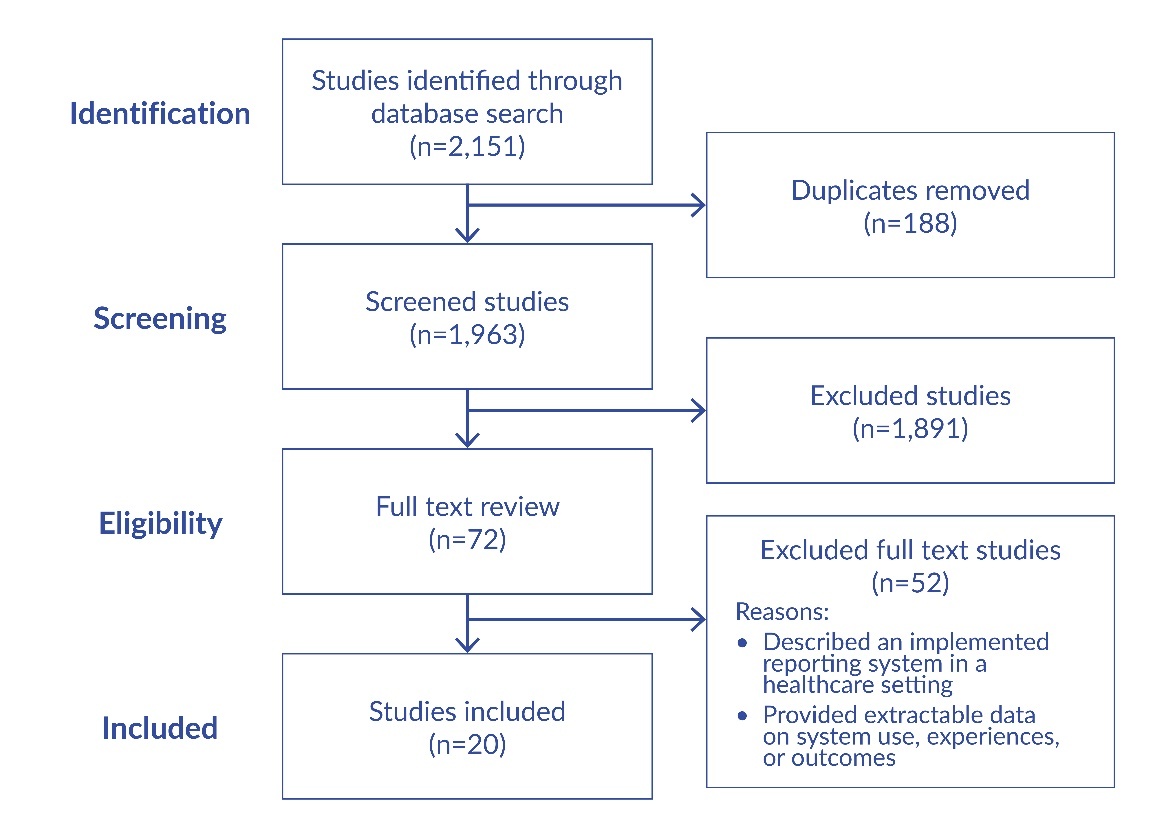
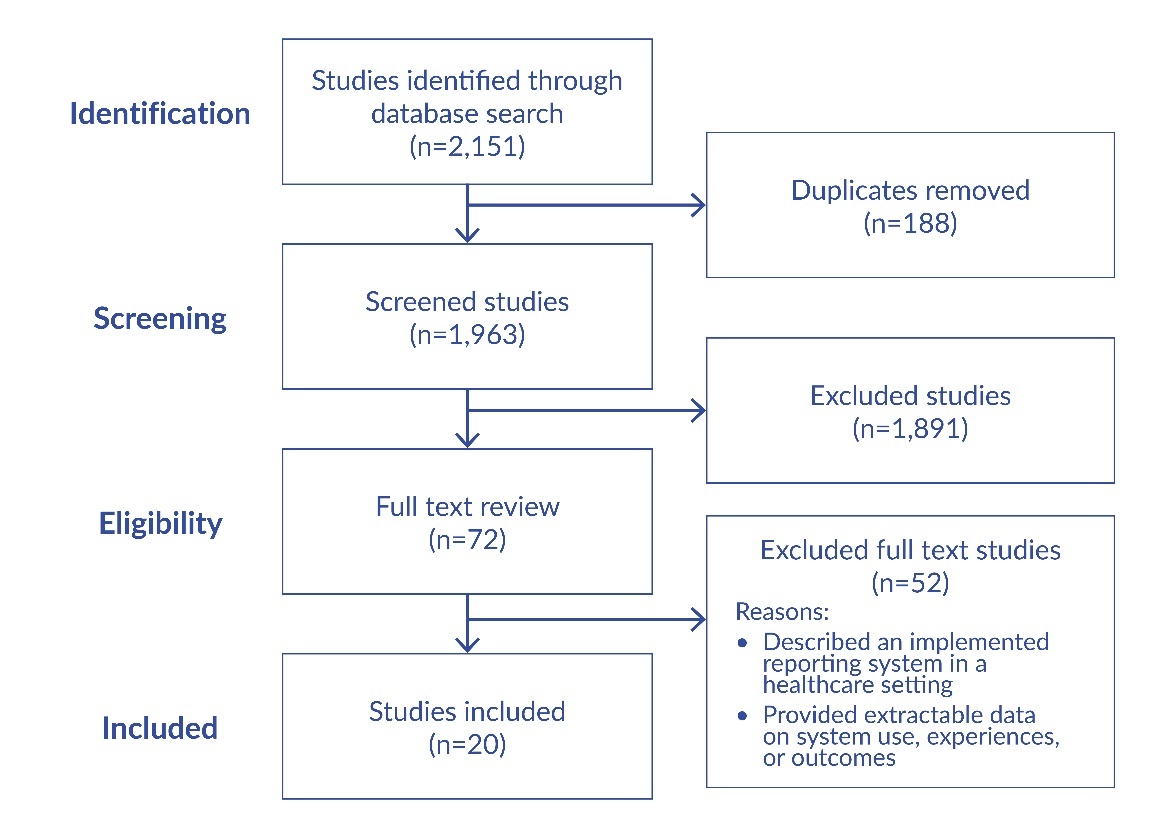
All identified citations were imported into Covidence, a systematic review tool, for deduplication and screening. Two reviewers (S.Q. and S.L.) independently screened all titles and abstracts for relevance. Full texts of potentially eligible articles were retrieved and reviewed in duplicate. Any disagreements were resolved through consensus or, when necessary, adjudicated by a third reviewer. After removing duplicates, 1,963 unique records were screened at the title and abstract level by two reviewers (S.Q. and S.L.) independently. Studies were included at this stage if they appeared to meet the eligibility criteria: empirical research (quantitative, qualitative, or mixed methods) on systems allowing patients or families to report safety concerns, near misses, or adverse events in healthcare settings, conducted across any healthcare environment (including hospitals, clinics, or long-term care facilities), published in English between January 2000 and May 2025. Articles that were clearly not empirical studies; focused exclusively on clinician-generated reports; solely evaluated patient satisfaction without a reporting component; or were opinion pieces, editorials, or abstracts without accessible full-text data were excluded.
After title and abstract screening, 72 articles were selected for full-text review. At this stage, the same inclusion and exclusion criteria were applied more stringently to the full texts. Each article was reviewed in detail to confirm that it: (1) described an implemented patient- or family-initiated reporting system for safety events in a healthcare setting, and (2) provided empirical data on the use, outcomes, or experience of such a system. Articles were excluded at this stage if, upon review, they did not meet all inclusion criteria, focused solely on staff-initiated reporting, or did not report empirical findings. Of the 72 full-text articles reviewed, 20 met all inclusion criteria and were included in the final synthesis (Figure 1). Because scoping reviews aim to map the breadth and conceptual terrain of a topic, we also included systematic reviews that met the eligibility criteria. These reviews were not treated as sources of pooled effect estimates but rather as higher-level syntheses used to contextualize primary studies, identify previously described themes, and highlight gaps in evaluation or implementation. This approach aligns with scoping review methodology and clarifies the analytic role of review articles within our evidence map.
Data extraction was performed using a standardized form to capture relevant information across multiple domains. Two reviewers independently extracted and cross-checked data to ensure accuracy. Extracted data were analyzed using narrative synthesis and organized into key thematic categories reflecting patterns in reporting mechanisms, engagement strategies, barriers and facilitators, and reported outcomes. The review process was iterative and reflexive, allowing for the refinement of themes as analysis progressed.
Results
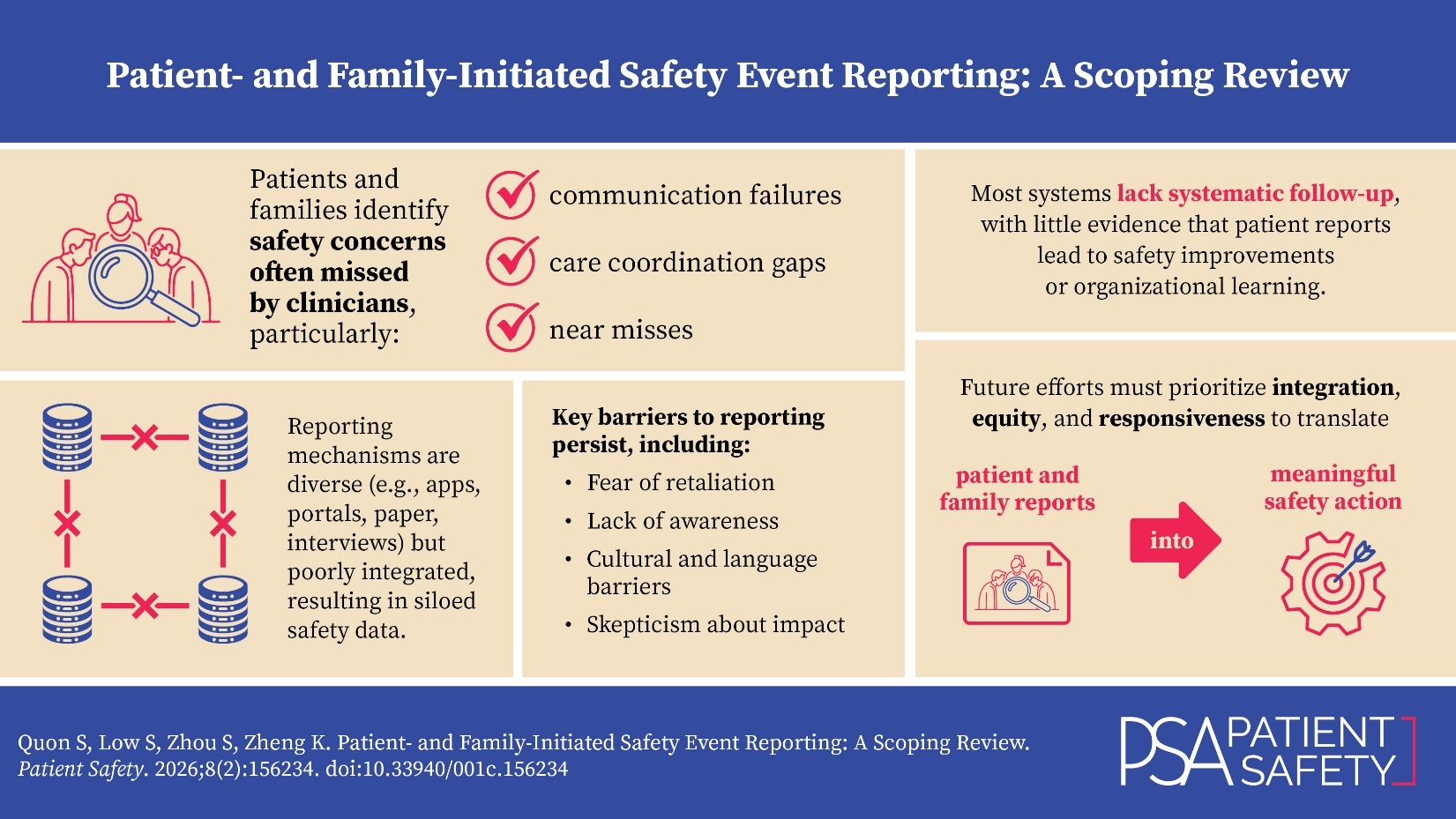
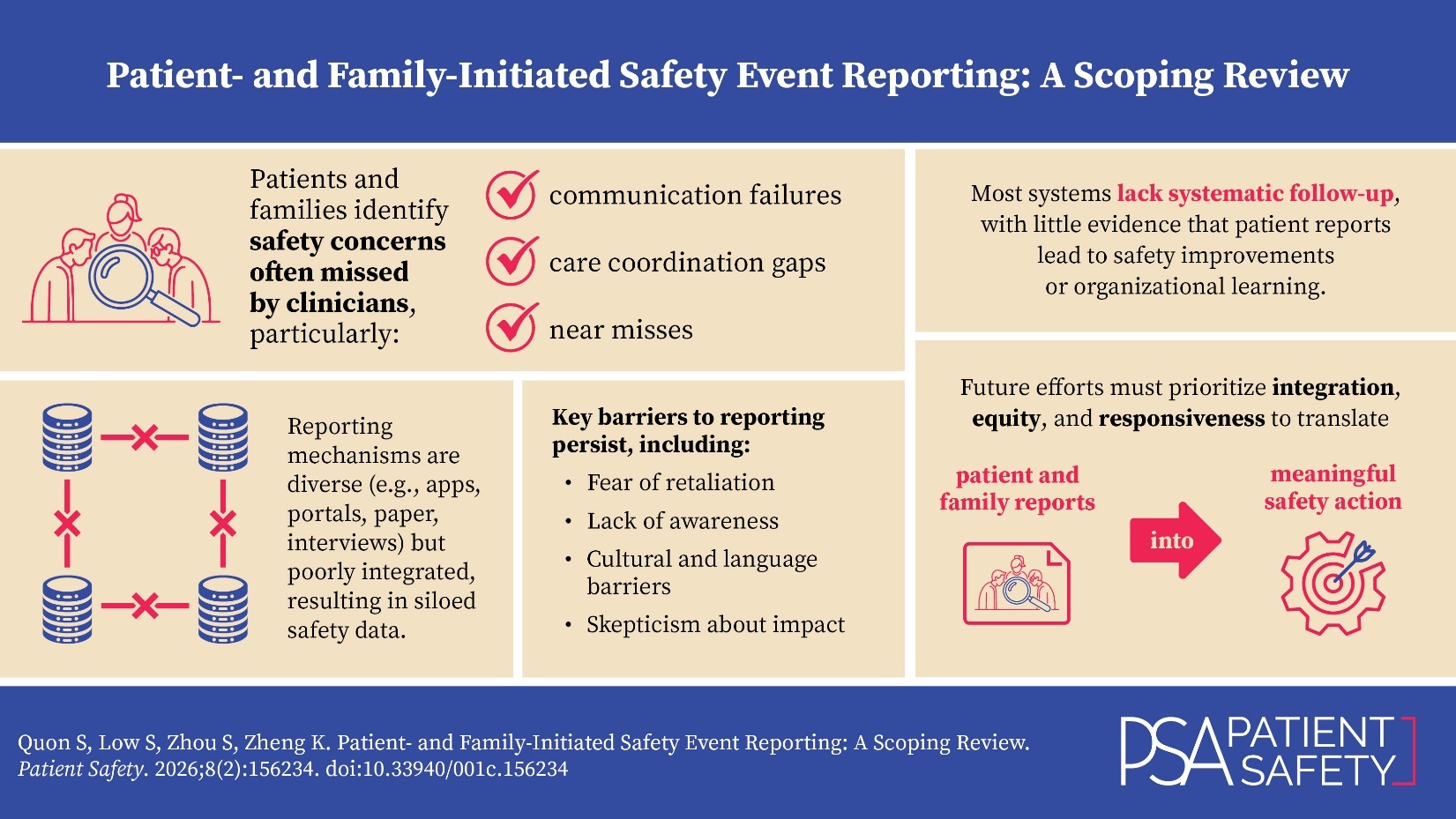
A total of 20 studies were included in this scoping review. Thematic analysis revealed four key themes regarding patient- and family-initiated safety event reporting systems: (1) diverse reporting mechanisms but limited integration, (2) unique safety concerns identified by patients and families, (3) barriers to engagement and reporting, and (4) limited evidence of systematic follow-up or demonstrated impact. Together, these themes highlight both the promise and persistent limitations of patient and family engagement in safety event reporting across healthcare settings. An overview of the 20 studies is provided in Table 1.
Theme 1: Diverse Reporting Mechanisms but Limited Integration
Patient- and family-initiated safety event reporting systems employ a range of modalities, including mobile apps, online portals, paper forms, hotlines, and in-person interviews. These diverse mechanisms broaden accessibility and enable multiple stakeholders—patients, families, and staff—to report safety concerns in real time.11,12,31 Such reports frequently identify communication lapses, near misses, and environmental hazards that are not captured by traditional clinician-led incident reporting systems.11,14,15,31
Despite these advantages, most systems remain siloed. Reports from different mechanisms are rarely integrated or cross-referenced, leading to fragmented data and missed opportunities for organizational learning.15,32 Without unified analysis across platforms, healthcare institutions risk underutilizing valuable patient-generated insights.32,33 Overall, while the range of reporting options facilitates engagement, the lack of systematic integration weakens their collective impact on safety improvement.11,12,32,33
Theme 2: Unique Safety Concerns Identified by Patients and Families
Patients and families contribute perspectives that often diverge from those of healthcare providers. Commonly reported concerns include communication failures, disrespectful interactions, diagnostic and therapeutic errors, delays in care, and medication issues.11,12,14–17,33–35 These events are frequently absent from staff-based reports and often reflect lapses in dignity, compassion, or coordination of care.
Patient and family reports not only highlight technical failures but also draw attention to system-level vulnerabilities, such as inadequate staffing, poor communication policies, and organizational barriers to safe care. The Society of Critical Care Medicine (SCCM) recommends incorporating these perspectives, particularly through interviews, into routine safety surveillance, noting that families often detect unique medication errors not captured through standard monitoring practices.36 Ultimately, patient and family reporting adds a vital dimension to understanding safety risks, emphasizing the centrality of respect, communication, and trust in preventing harm.
Theme 3: Barriers to Engagement and Reporting
Despite the value of patient and family reporting, several barriers limit participation. A lack of awareness and understanding about what constitutes a reportable event is a common issue, particularly among those unfamiliar with clinical deterioration or escalation protocols.37,38 Reporting systems that are complex or perceived as burdensome further discourage engagement.12,38
Patients and families also express concerns about potential retaliation or being labeled as “difficult,” especially in hierarchical healthcare environments.7,39 Some doubt whether their reports will lead to meaningful change, which reduces motivation to engage.38,39 Additional barriers include language and cultural differences, limited health literacy, and discomfort in questioning providers due to perceived authority gradients.7,12 Addressing these issues requires simplifying reporting systems, improving education, ensuring non-retaliation, and visibly responding to patient concerns to build a culture of trust and safety.37–39
Theme 4: Limited Evidence of Systematic Follow-Up or Impact
While the feasibility and value of patient- and family-initiated reporting are well established, there is limited evidence of systematic follow-up or measurable impact on patient safety outcomes. Studies consistently show that such reports identify unique safety issues,11,12,15,40 yet it remains unclear whether these insights translate into organizational learning or quality improvement.
Systematic reviews reinforce this concern. For instance, it was found that engagement definitions and processes vary widely and that empirical evidence of real-world outcomes is lacking.18 Other studies similarly emphasize the need for consensus guidelines and more robust evaluation frameworks.2 It was also highlighted that most incident reporting systems fail to demonstrate clear links between data collection and improved outcomes.41 Even high-level recommendations, such as the SCCM’s guideline on medication safety, advocate for patient- and family-reported outcomes but do not offer evidence of follow-through or impact.36 Thus, while patient and family reporting systems offer valuable data, their effectiveness in driving safety improvements remains largely unproven.2,18,41
Discussion
This scoping review synthesizes evidence from 20 studies on the implementation, use, and impact of patient- and family-initiated safety event reporting systems in healthcare. Four key themes emerged: the presence of diverse but poorly integrated reporting mechanisms, the identification of unique safety concerns by patients and families, the persistence of barriers to engagement and reporting, and a lack of evidence for systematic follow-up or demonstrated impact. These findings reinforce the complementary role that patients and families can play in patient safety while highlighting the systemic and structural challenges that limit the effectiveness of these reporting systems.
Although reporting mechanisms have diversified in recent years—ranging from paper forms to mobile apps and digital platforms—these systems often operate in silos, with minimal integration or cross-referencing between reporting streams.11,12,32 As a result, healthcare organizations may be capturing valuable insights from patients and families without synthesizing this data alongside traditional clinician-reported incidents or using it to guide systemwide safety improvements. Without formal processes for aggregating and analyzing patient-generated data, these efforts risk being perceived as symbolic rather than impactful.14,33,42
Notably, patients and families report a broader range of concerns than clinicians—often identifying interpersonal issues, communication breakdowns, and failures in compassion or dignity that fall outside the scope of conventional adverse event reporting systems.15,16,35 These reports provide a richer understanding of how patients experience safety and harm, yet they are often undervalued or excluded from formal safety reviews. Guidelines from professional bodies such as the SCCM recommend incorporating family perspectives into safety surveillance, particularly in areas such as medication error detection,36 but operational models to support this integration remain underdeveloped.
Engagement is further constrained by a range of barriers, including lack of knowledge, concerns about retaliation, and cultural and language obstacles.7,39,43 Patients and families are often hesitant to question authority or report concerns if they perceive healthcare providers as too busy or if they fear their care will be negatively affected. These dynamics are compounded by healthcare hierarchies and inequities in access to information. Addressing these barriers requires more than just technical fixes—it necessitates a shift in organizational culture toward one that values and protects the contributions of patients and families.37
A key limitation identified across the literature is the lack of evidence that patient and family reports lead to meaningful outcomes. Most studies focus on feasibility or descriptive analysis, with few demonstrating follow-up actions, system-level learning, or improved patient safety metrics.2,18,41 This disconnect raises concerns about tokenism and missed opportunities to close feedback loops. It also reflects broader challenges in safety reporting systems, which often emphasize collection over application. To harness the full value of patient-reported safety data, future research must move beyond documentation to explore how these reports can trigger actionable change.
This review is subject to several limitations. First, it included only peer-reviewed studies published in English, which may exclude innovative non-English or gray literature sources. Second, the heterogeneity in study design, setting, and definitions of reporting limited direct comparisons. Additionally, many included studies were pilot projects or exploratory evaluations, with limited longitudinal or outcome-based data. Future research should focus on evaluating the impact of patient and family reporting systems using rigorous, longitudinal designs. There is also a need for the development of standardized frameworks and consensus guidelines that define best practices for integrating, responding to, and learning from patient-generated safety data. Furthermore, future studies should explore how engagement can be made equitable, inclusive, and sustainable across diverse populations and care settings.
Conclusion
Patient- and family-initiated safety event reporting systems represent a promising strategy for advancing patient-centered care and enhancing safety surveillance. These systems capture distinct safety concerns often missed by clinicians, particularly those related to communication, respect, and coordination. However, despite their potential, the impact of these systems is undermined by fragmented implementation, cultural and practical barriers to engagement, and a lack of evidence that reports are systematically followed up or lead to improvements in safety outcomes. To move forward, healthcare organizations must invest in infrastructure that supports integration, responsiveness, and equity in safety reporting. Importantly, they must also demonstrate that patient and family voices are not only heard but meaningfully acted upon. Bridging the gap between patient input and system learning is essential to building a truly safe and inclusive healthcare system.
Disclosures
The authors declare that they have no relevant or material financial interests. AI was not used in the writing or analysis in this manuscript.
About the Authors
Stephanie Quon (stephaniesfquon@gmail.com) is a medical student at the University of British Columbia, Vancouver, Canada.
Sarah Low is a Master of Public Health student at the University of British Columbia, Vancouver, Canada.
Sarah Zhou is a medical student at the University of British Columbia, Vancouver, Canada.
Katherine Zheng is a family physician in Vancouver, Canada.